Downloaded 194 times
![2. THYROID HORMONES:
Hyperthyroid individuals are more lileky to
have PE, & with reversion to a euthyroid state,
the rate of PE dropped
At present, role of hormones in the genesis of
PE is not completely understood.
[Gorona et al, 2004]
PATHOPHYSIOLOGY OF PE](https://image.slidesharecdn.com/prematureejaculation-161001111731/85/Premature-ejaculation-25-320.jpg)
![CHRONIC PROSTATITIS:
Chronic prostatitis is more prevalent among
men with a diagnosis of PE.
After 1 month of antibiotic treatment, most of
treated patients show a significant increase in
their IELT.
Mechanism behind link between chronic
prostatitis and PE and the mean by which
antibiotic treatment improved IELT are unclear.
[Janinni E. et al 2002]
PATHOPHYSIOLOGY OF PE](https://image.slidesharecdn.com/prematureejaculation-161001111731/85/Premature-ejaculation-28-320.jpg)
![ Other Behavioral therapy:
Precoitus masturbation partially desensitizes the
penis and leads to a delay in ejaculation.
It may be helpful for younger men suffering from
PE,
[Sadeghi-Nejad and Watson, 2008].](https://image.slidesharecdn.com/prematureejaculation-161001111731/85/Premature-ejaculation-39-320.jpg)
![ Must be given for 1 to 2 weeks to be effective in
PE.
Short-term adverse effects are yawning, nausea,
excessive sweating and fatigue.
Long-term adverse effects are loss of bone
density, reduced libido and erectile rigidity.
Adverse effects usually present at the beginning
of the treatment and they tend to disappear
within 2–3 weeks
[McMahon et al. 2004]
TREATMENT](https://image.slidesharecdn.com/prematureejaculation-161001111731/85/Premature-ejaculation-41-320.jpg)
![3-Dapoxetine
Dapoxetine is the only licensed drug in the
treatment of PE
A highly potent inhibitor of serotonin reuptake
transporter .
Following oral administration, it is rapidly
absorbed
After reaching T max, serum concentration
declines rapidly.
At 60 mg dose: T max = 1.2 hr
No interaction when used with food or PDE5
inhibitors.
[Feige et al. 2011]](https://image.slidesharecdn.com/prematureejaculation-161001111731/85/Premature-ejaculation-43-320.jpg)
![4. Tramadol:
A centrally acting synthetic opioid analgesic.
Its mechanism of action in PE is poorly
understood
In 2009 Safarinejad and Hosseini have published
a randomized, controlled trial on the use of
tramadol HCL to treat PE [Safarinejad and Hosseini, 2009].
Various research groups have shown tramadol to
have some efficacy in treating PE
[Alghobary et al. 2010]
TREATMENT](https://image.slidesharecdn.com/prematureejaculation-161001111731/85/Premature-ejaculation-45-320.jpg)
![ It has two mechanisms of action. It exerts an
effect on the μ-opioid receptor and also inhibits
noradrenaline and serotonin reuptake.
On demand tramadol 50mg taken 2 hours before
intercourse.
[Salem et al. 2008]](https://image.slidesharecdn.com/prematureejaculation-161001111731/85/Premature-ejaculation-46-320.jpg)
![Phosphodiesterase 5 Inhibitors:
The role of PDE5 inhibitors (PDE5-I) in the
management of PE is controversial.
Mechanisms of action: 1) A central effect
increased NO and reduced sympathetic tone, 2)
smooth muscle dilatation of vas deferens and
seminal vesicles.
[Wang et al. 2007]](https://image.slidesharecdn.com/prematureejaculation-161001111731/85/Premature-ejaculation-47-320.jpg)
![III. TOPICAL AGENTS:
1. Severance Secret Cream(SS Cream):
Made of the extracts of nine natural products.
Applied to the glans penis 1hr before and washed
off immediately prior to coitus.
Stopwatch-IELT increase.
The main disadvantage of SS-cream is an
unpleasant odor, which makes it unpalatable to
many patients.
[Xin et al. 2000]
TREATMENT](https://image.slidesharecdn.com/prematureejaculation-161001111731/85/Premature-ejaculation-48-320.jpg)
![ A recently developed topical aerosol for PE known
as (PSD-502) is delivered combination of
lidocaine and prilocaine designed for use in PE.
Can penetrate the glans within 5–10 min, and
can’t penetrate intact keratinised skin so not
anaesthetize the shaft of the penis or the hands
[Carson and Wyllie, 2010]
TREATMENT](https://image.slidesharecdn.com/prematureejaculation-161001111731/85/Premature-ejaculation-50-320.jpg)

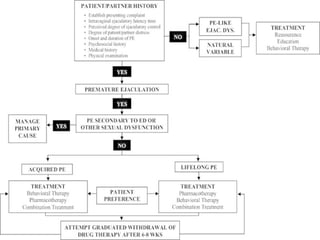


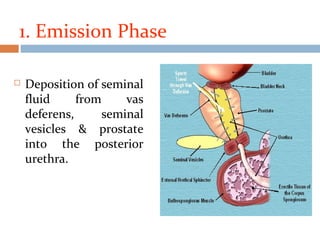
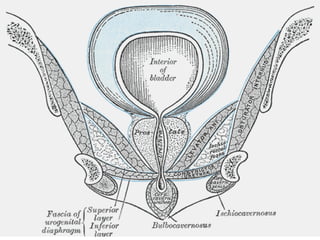
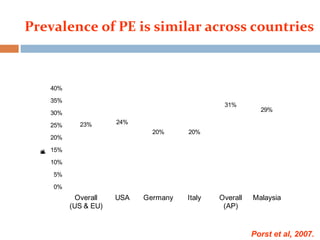
Ejaculation involves three phases - emission, bladder neck contraction, and expulsion. Premature ejaculation (PE) is defined as ejaculation occurring within about 1 minute of penetration that the man has little control over, causing distress. The pathophysiology of PE is not fully understood but may involve genetic, psychological, hormonal, penile sensitivity, and prostatic factors. PE is diagnosed based on history and can be evaluated using tools like the Premature Ejaculation Diagnostic Tool. Treatment includes behavioral therapies like stop-start and squeeze techniques as well as pharmacotherapies.























![Erectile Dysfunction [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/ededmond-140716212750-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)