Downloaded 352 times
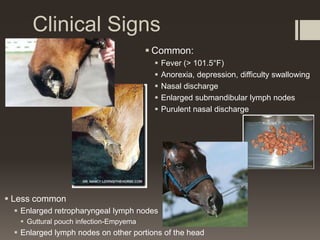
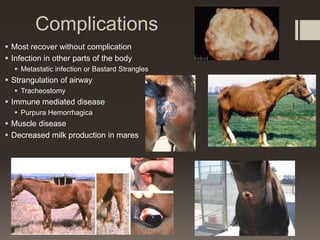




Strangles is a highly contagious bacterial infection caused by Streptococcus equi subspecies equi that commonly affects young horses. It primarily causes fever and swelling of the lymph nodes in the head and neck. While most horses recover without complications, the disease can spread easily through nasal discharge from infected or carrier horses. Proper outbreak management includes isolation of sick horses, thorough disinfection, and vaccination to help control spread.