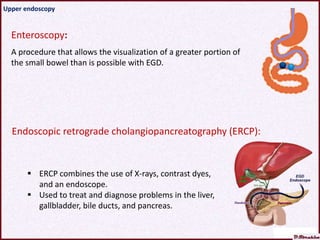
The document discusses the diagnosis of parasitic diseases, detailing various approaches including clinical diagnosis, laboratory investigations, and imaging techniques such as endoscopy. It outlines specific endoscopic procedures and their uses, including upper and lower endoscopy, as well as various parasitic infections that can be diagnosed through these methods. The text emphasizes the diagnostic and therapeutic value of endoscopy despite its invasive nature and potential complications.