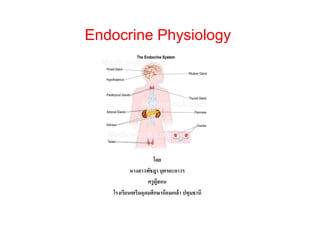
The endocrine system is a messenger system comprising feedback loops of the hormones released by internal glands of an organism directly into the circulatory system, regulating distant target organs. In vertebrates, the hypothalamus is the neural control center for all endocrine systems.
The endocrine system is a messenger system comprising feedback loops of the hormones released by internal glands of an organism directly into the circulatory system, regulating distant target organs. In vertebrates, the hypothalamus is the neural control center for all endocrine systems.
Glucagon (The Guyton and Hall physiology)Maryam Fida
GLUCAGON
Secreted by Alpha cells of Islets of Langerhans when the blood glucose concentration falls.
Also called hyperglycemic hormone
Antagonistic to those of insulin.
Increases blood sugar level, increases peripheral utilization of lipids and conversion of proteins into glucose.
Glucose is the only nutrient that normally can be used by the brain, retina and germinal epithelium of the gonads.
Effect of Glucagon on CHO metabolism
Anabolic
It increases blood glucose level.
It increases glycogenolysis in liver.
It increases Gluconeogenesis
ACTION OF GLUCAGON ON LIPID METABOLISM
Catabolic Effect
It activates adipose cell lipase which liberates fatty acids for energy utilization.
It also inhibits the storage of triglycerides in the liver.
Effect of Glucagon on PROTEIN metabolism
Catabolic effect
Increase transport of amino acid in to liver cells
These amino acids are used for gluconeogenesis.
Other Effects
It also increases the strength of the heart
Increases blood flow to some organs such as kidneys
Enhances bile secretion
Inhibits gastric acid secretion
Factors Increase
Glucagon Secretion
Factors decrease
Glucagon Secretion
FACTORS STIMULATING SOMATOSTATIN SECRETIONACTIONS OF SOMATOSTATIN
Reabsorption In Renal Tubule (The Guyton and Hall physiology)Maryam Fida
Features of PCTPCT have high capacity of active & passive re-absorption.
This is due to special cellular features of epithelial cells.
They have increased no. of mitochondria due to high metabolic activity.
brush border on luminal (apical) side.
Brush border contains protein carrier molecules to transport Na+ by co-transport mechanism with other substances (a.acids, glucose etc).
Additional sodium is transported by COUNTER-TRANSPORT that reabsorb sodium while secreting hydrogen.
About 65 % of filtered load of Na+ & water is reabsorbed in PCT.
A lower % age of Cl- is also absorbed.
In 1st half of PC tubules, Na+ is re-absorbed by co-transport along with glucose, a.acids and other solutes.
In 2nd half of PC tubules, mainly Na+ is reabsorbed with Cl- and some of glucose + a.acids remain un-absorbed.
2nd half of PCT has high conc of Cl- (140 mEq/L) as compared to 1st half (105 mEq/L).
Glucagon (The Guyton and Hall physiology)Maryam Fida
GLUCAGON
Secreted by Alpha cells of Islets of Langerhans when the blood glucose concentration falls.
Also called hyperglycemic hormone
Antagonistic to those of insulin.
Increases blood sugar level, increases peripheral utilization of lipids and conversion of proteins into glucose.
Glucose is the only nutrient that normally can be used by the brain, retina and germinal epithelium of the gonads.
Effect of Glucagon on CHO metabolism
Anabolic
It increases blood glucose level.
It increases glycogenolysis in liver.
It increases Gluconeogenesis
ACTION OF GLUCAGON ON LIPID METABOLISM
Catabolic Effect
It activates adipose cell lipase which liberates fatty acids for energy utilization.
It also inhibits the storage of triglycerides in the liver.
Effect of Glucagon on PROTEIN metabolism
Catabolic effect
Increase transport of amino acid in to liver cells
These amino acids are used for gluconeogenesis.
Other Effects
It also increases the strength of the heart
Increases blood flow to some organs such as kidneys
Enhances bile secretion
Inhibits gastric acid secretion
Factors Increase
Glucagon Secretion
Factors decrease
Glucagon Secretion
FACTORS STIMULATING SOMATOSTATIN SECRETIONACTIONS OF SOMATOSTATIN
Reabsorption In Renal Tubule (The Guyton and Hall physiology)Maryam Fida
Features of PCTPCT have high capacity of active & passive re-absorption.
This is due to special cellular features of epithelial cells.
They have increased no. of mitochondria due to high metabolic activity.
brush border on luminal (apical) side.
Brush border contains protein carrier molecules to transport Na+ by co-transport mechanism with other substances (a.acids, glucose etc).
Additional sodium is transported by COUNTER-TRANSPORT that reabsorb sodium while secreting hydrogen.
About 65 % of filtered load of Na+ & water is reabsorbed in PCT.
A lower % age of Cl- is also absorbed.
In 1st half of PC tubules, Na+ is re-absorbed by co-transport along with glucose, a.acids and other solutes.
In 2nd half of PC tubules, mainly Na+ is reabsorbed with Cl- and some of glucose + a.acids remain un-absorbed.
2nd half of PCT has high conc of Cl- (140 mEq/L) as compared to 1st half (105 mEq/L).
KEY CONCEPTS
45.1 Hormones and other signaling molecules bind to target
receptors, triggering specific response pathways
45.2 Feedback regulation and coordination with the nervous system are common in endocrine signaling
45.3 Endocrine glands respond to diverse stimuli in regulating homeostasis, development,
and behavior
22.chemical control & coordination in one shot.pptxanonymous
There are special chemicals which act as hormones and provide chemical
coordination, integration and regulation in the human body. These hormones
regulate metabolism, growth and development of our organs, the endocrine glands
or certain cells. The endocrine system is composed of hypothalamus, pituitary
and pineal, thyroid, adrenal, pancreas, parathyroid, thymus and gonads (testis
and ovary). In addition to these, some other organs, e.g., gastrointestinal tract,
kidney, heart etc., also produce hormones. Progesterone plays a major role in the maintenance of pregnancy as
well as in mammary gland development and lactation. The atrial wall of the heart
produces atrial natriuretic factor which decreases the blood pressure. Kidney
produces erythropoietin which stimulates erythropoiesis. The gastrointestinal tract
secretes gastrin, secretin, cholecystokinin and gastric inhibitory peptide. These
hormones regulate the secretion of digestive juices and help in digestion.
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journeygreendigital
Tom Selleck, an enduring figure in Hollywood. has captivated audiences for decades with his rugged charm, iconic moustache. and memorable roles in television and film. From his breakout role as Thomas Magnum in Magnum P.I. to his current portrayal of Frank Reagan in Blue Bloods. Selleck's career has spanned over 50 years. But beyond his professional achievements. fans have often been curious about Tom Selleck Health. especially as he has aged in the public eye.
Follow us on: Pinterest
Introduction
Many have been interested in Tom Selleck health. not only because of his enduring presence on screen but also because of the challenges. and lifestyle choices he has faced and made over the years. This article delves into the various aspects of Tom Selleck health. exploring his fitness regimen, diet, mental health. and the challenges he has encountered as he ages. We'll look at how he maintains his well-being. the health issues he has faced, and his approach to ageing .
Early Life and Career
Childhood and Athletic Beginnings
Tom Selleck was born on January 29, 1945, in Detroit, Michigan, and grew up in Sherman Oaks, California. From an early age, he was involved in sports, particularly basketball. which played a significant role in his physical development. His athletic pursuits continued into college. where he attended the University of Southern California (USC) on a basketball scholarship. This early involvement in sports laid a strong foundation for his physical health and disciplined lifestyle.
Transition to Acting
Selleck's transition from an athlete to an actor came with its physical demands. His first significant role in "Magnum P.I." required him to perform various stunts and maintain a fit appearance. This role, which he played from 1980 to 1988. necessitated a rigorous fitness routine to meet the show's demands. setting the stage for his long-term commitment to health and wellness.
Fitness Regimen
Workout Routine
Tom Selleck health and fitness regimen has evolved. adapting to his changing roles and age. During his "Magnum, P.I." days. Selleck's workouts were intense and focused on building and maintaining muscle mass. His routine included weightlifting, cardiovascular exercises. and specific training for the stunts he performed on the show.
Selleck adjusted his fitness routine as he aged to suit his body's needs. Today, his workouts focus on maintaining flexibility, strength, and cardiovascular health. He incorporates low-impact exercises such as swimming, walking, and light weightlifting. This balanced approach helps him stay fit without putting undue strain on his joints and muscles.
Importance of Flexibility and Mobility
In recent years, Selleck has emphasized the importance of flexibility and mobility in his fitness regimen. Understanding the natural decline in muscle mass and joint flexibility with age. he includes stretching and yoga in his routine. These practices help prevent injuries, improve posture, and maintain mobilit
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...VarunMahajani
Disruption of blood supply to lung alveoli due to blockage of one or more pulmonary blood vessels is called as Pulmonary thromboembolism. In this presentation we will discuss its causes, types and its management in depth.
Knee anatomy and clinical tests 2024.pdfvimalpl1234
This includes all relevant anatomy and clinical tests compiled from standard textbooks, Campbell,netter etc..It is comprehensive and best suited for orthopaedicians and orthopaedic residents.
Title: Sense of Taste
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the structure and function of taste buds.
Describe the relationship between the taste threshold and taste index of common substances.
Explain the chemical basis and signal transduction of taste perception for each type of primary taste sensation.
Recognize different abnormalities of taste perception and their causes.
Key Topics:
Significance of Taste Sensation:
Differentiation between pleasant and harmful food
Influence on behavior
Selection of food based on metabolic needs
Receptors of Taste:
Taste buds on the tongue
Influence of sense of smell, texture of food, and pain stimulation (e.g., by pepper)
Primary and Secondary Taste Sensations:
Primary taste sensations: Sweet, Sour, Salty, Bitter, Umami
Chemical basis and signal transduction mechanisms for each taste
Taste Threshold and Index:
Taste threshold values for Sweet (sucrose), Salty (NaCl), Sour (HCl), and Bitter (Quinine)
Taste index relationship: Inversely proportional to taste threshold
Taste Blindness:
Inability to taste certain substances, particularly thiourea compounds
Example: Phenylthiocarbamide
Structure and Function of Taste Buds:
Composition: Epithelial cells, Sustentacular/Supporting cells, Taste cells, Basal cells
Features: Taste pores, Taste hairs/microvilli, and Taste nerve fibers
Location of Taste Buds:
Found in papillae of the tongue (Fungiform, Circumvallate, Foliate)
Also present on the palate, tonsillar pillars, epiglottis, and proximal esophagus
Mechanism of Taste Stimulation:
Interaction of taste substances with receptors on microvilli
Signal transduction pathways for Umami, Sweet, Bitter, Sour, and Salty tastes
Taste Sensitivity and Adaptation:
Decrease in sensitivity with age
Rapid adaptation of taste sensation
Role of Saliva in Taste:
Dissolution of tastants to reach receptors
Washing away the stimulus
Taste Preferences and Aversions:
Mechanisms behind taste preference and aversion
Influence of receptors and neural pathways
Impact of Sensory Nerve Damage:
Degeneration of taste buds if the sensory nerve fiber is cut
Abnormalities of Taste Detection:
Conditions: Ageusia, Hypogeusia, Dysgeusia (parageusia)
Causes: Nerve damage, neurological disorders, infections, poor oral hygiene, adverse drug effects, deficiencies, aging, tobacco use, altered neurotransmitter levels
Neurotransmitters and Taste Threshold:
Effects of serotonin (5-HT) and norepinephrine (NE) on taste sensitivity
Supertasters:
25% of the population with heightened sensitivity to taste, especially bitterness
Increased number of fungiform papillae
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
Couples presenting to the infertility clinic- Do they really have infertility...Sujoy Dasgupta
Dr Sujoy Dasgupta presented the study on "Couples presenting to the infertility clinic- Do they really have infertility? – The unexplored stories of non-consummation" in the 13th Congress of the Asia Pacific Initiative on Reproduction (ASPIRE 2024) at Manila on 24 May, 2024.
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
Recomendações da OMS sobre cuidados maternos e neonatais para uma experiência pós-natal positiva.
Em consonância com os ODS – Objetivos do Desenvolvimento Sustentável e a Estratégia Global para a Saúde das Mulheres, Crianças e Adolescentes, e aplicando uma abordagem baseada nos direitos humanos, os esforços de cuidados pós-natais devem expandir-se para além da cobertura e da simples sobrevivência, de modo a incluir cuidados de qualidade.
Estas diretrizes visam melhorar a qualidade dos cuidados pós-natais essenciais e de rotina prestados às mulheres e aos recém-nascidos, com o objetivo final de melhorar a saúde e o bem-estar materno e neonatal.
Uma “experiência pós-natal positiva” é um resultado importante para todas as mulheres que dão à luz e para os seus recém-nascidos, estabelecendo as bases para a melhoria da saúde e do bem-estar a curto e longo prazo. Uma experiência pós-natal positiva é definida como aquela em que as mulheres, pessoas que gestam, os recém-nascidos, os casais, os pais, os cuidadores e as famílias recebem informação consistente, garantia e apoio de profissionais de saúde motivados; e onde um sistema de saúde flexível e com recursos reconheça as necessidades das mulheres e dos bebês e respeite o seu contexto cultural.
Estas diretrizes consolidadas apresentam algumas recomendações novas e já bem fundamentadas sobre cuidados pós-natais de rotina para mulheres e neonatos que recebem cuidados no pós-parto em unidades de saúde ou na comunidade, independentemente dos recursos disponíveis.
É fornecido um conjunto abrangente de recomendações para cuidados durante o período puerperal, com ênfase nos cuidados essenciais que todas as mulheres e recém-nascidos devem receber, e com a devida atenção à qualidade dos cuidados; isto é, a entrega e a experiência do cuidado recebido. Estas diretrizes atualizam e ampliam as recomendações da OMS de 2014 sobre cuidados pós-natais da mãe e do recém-nascido e complementam as atuais diretrizes da OMS sobre a gestão de complicações pós-natais.
O estabelecimento da amamentação e o manejo das principais intercorrências é contemplada.
Recomendamos muito.
Vamos discutir essas recomendações no nosso curso de pós-graduação em Aleitamento no Instituto Ciclos.
Esta publicação só está disponível em inglês até o momento.
Prof. Marcus Renato de Carvalho
www.agostodourado.com
ARTIFICIAL INTELLIGENCE IN HEALTHCARE.pdfAnujkumaranit
Artificial intelligence (AI) refers to the simulation of human intelligence processes by machines, especially computer systems. It encompasses tasks such as learning, reasoning, problem-solving, perception, and language understanding. AI technologies are revolutionizing various fields, from healthcare to finance, by enabling machines to perform tasks that typically require human intelligence.
- Video recording of this lecture in English language: https://youtu.be/lK81BzxMqdo
- Video recording of this lecture in Arabic language: https://youtu.be/Ve4P0COk9OI
- Link to download the book free: https://nephrotube.blogspot.com/p/nephrotube-nephrology-books.html
- Link to NephroTube website: www.NephroTube.com
- Link to NephroTube social media accounts: https://nephrotube.blogspot.com/p/join-nephrotube-on-social-media.html
2. Endocrine vs. Nervous System
• Major communication systems in the body
• Integrate stimuli and responses to changes
in external and internal environment
• Both are crucial to coordinated functions of
highly differentiated cells, tissues and
organs
• Unlike the nervous system, the endocrine
system is anatomically discontinuous.
3. Introduction
• The endocrine system includes the organs of the body
that secrete hormones directly into body fluids such
as blood
– Regulates chemical reaction in cells and therefore control
functions of the organs, tissues, and other cells
bloodstream
to
Glands
into
secrete
hormones
34-3
target tissues
4. Hormones
• Endocrine glands
– Ductless
– Release hormones
• Directly into target tissues
• Into bloodstream to be carried to target tissues
• Hormones – chemicals secreted by a cell
that affect the functions of other cells
34-4
5. Hormones (cont.)
• Many are derived from steroids that easily
cross the cell membrane
• Examples of steroid hormones
–
–
–
–
Estrogen
Progesterone
Testosterone
Cortisol
hormones
34-5
6. Hormones (cont.)
• Nonsteroidal hormones
• Prostaglandins
– Made of amino acids or
proteins and cannot cross the
cell membrane easily
– Local, or tissue, hormones
– Derived from lipid molecules
– Do not travel in the
bloodstream
– Target tissues are located close
by
– Produced by organs such as
– Bind to receptors on the
surface of the cells
– G-protein – activated by the
hormone-receptor complex
•
•
•
•
•
• Activates enzymes inside cell
34-6
Kidneys
Heart
Stomach
Uterus
Brain
7. Negative and Positive
Feedback Loops
• Control hormone levels
• Negative feedback loop
– Hormone release stops in response to decrease
in stimulus
• Stimulus (eating) raises blood glucose levels
• Pancreas releases insulin in response to elevated
blood glucose
• Blood glucose decreases as it is used by the body or
stored in the liver
• Insulin release stops as blood glucose levels
normalize
34-7
8. Negative and Positive
Feedback Loops (cont.)
• Positive feedback loop
– As long as stimulus is present, action of
hormone continues
• Infant nursing at mother’s breast stimulates
hypothalamus stimulates posterior pituitary
• Oxytocin released stimulates milk production and
ejection from mammary glands
• Milk release continues as long as infant continues to
nurse
34-8
9. Apply Your Knowledge
Match the following:
ANSWER:
___ Chemicals that effect cell function A. Nonsteroidal hormone
E
B
___ Easily cross cell membranes
B. Steroidal hormone
A
___ Made of amino acids
C. G-protein
D
___ Target nearby cells
D. Prostaglandins
___ Activated by hormone-receptor
C
complex
E. Hormones
___ Cannot cross cell membranes easily
A
B
___ Estrogen and cortisol
34-9
10. Hypothalamus
• Hormones
– Oxytocin
– Antidiuretic hormone (ADH)
• Hormones transported to the posterior
pituitary for storage
• Directs posterior pituitary to release
hormones
34-10
Glands
11. Pituitary Gland
• Controlled by the hypothalamus
• Located at the base of the brain
– Protected by a bony structure called the sella turcica
– The optic chiasm is located just above the pituitary gland
• Carries visual information to the brain for interpretation
• Two lobes
– Anterior lobe
– Posterior lobe
Glands
34-11
12. Pituitary Gland (cont.)
Growth hormone
Stimulates increase in size
of muscles and bones
Luteinizing
Prolactin Stimulates milk
production
Anterior
Lobe
Females: stimulates ovulation
and estrogen production
Males: stimulates testosterone production
Adrenocorticotropic
Stimulates the adrenal cortex
to release its hormones
Thyroid-stimulating
Stimulates the thyroid
gland to release its
hormones
Follicle-stimulating
Females: stimulates estrogen
production and maturation of the ova
Males: stimulates sperm production
34-12
13. Pituitary Gland (cont.)
Oxytocin
Posterior
Lobe
Antidiuretic hormone (ADH)
Stimulates the kidneys to
conserve water
34-13
Females: causes
contraction of the
uterus and ejection of
breast milk
Males: stimulates
contraction of the
prostate and vas
deferens during
sexual arousal
14. Apply Your Knowledge
Match the following:
ANSWER:
D, E Stored in posterior pituitary
___
A. Follicle-stimulating hormone
___ Milk production
B
B. Prolactin
D, E Produced by hypothalmus
___
C. Luteinizing hormone
___ Stimulates sperm production
A
D. ADH
___ Maturation of ova
A
E. Oxytocin
___ Stimulates ovulation
C
Super!
___ Conservation of water
D
___ Production of testosterone
C
___ Contraction of uterus
E
34-14
15. Thyroid Gland and
Parathyroid Glands
Thyroid Gland
Located below the larynx
Divided into follicles that store some of the hormones
Major hormones
T3 T4
Stimulate protein synthesis and
increase cellular energy
production
Lowers blood calcium levels
by activating osteoblasts that
Glands
build new bone tissue
34-15
16. Thyroid Gland and
Parathyroid Glands (cont.)
• Parathyroid glands
– Four located on the posterior surface of the thyroid
gland
– Secrete parathyroid hormone (PTH)
• Agonist to calcitonin by raising blood calcium levels
through activation of osetoclasts (dissolve bone)
– As bone dissolves, calcium levels in blood increase
Glands
34-16
17. 34-17
Apply Your Knowledge
True or False:
ANSWER:
__ Thyroid hormones stimulate protein synthesis.
T
Thyroid follicles store
__ The thyroid gland does not store hormones. some hormones.
F
__ PTH activates osteoblasts.
F
PTH activates osteoclasts.
__ Calcitonin increases cellular energy production.
F
Thyroid hormone
increases cellular
energy production.
T
__ The four parathyroid glands are located on the thyroid gland.
__ Calcitonin lowers blood calcium levels.
T
18. Adrenal Glands
• Located on top of each kidney
• Divided into the adrenal medulla and adrenal cortex
• Adrenal medulla
– Central portion
– Hormones
• Epinephrine
• Norepinephrine
• Same effects as sympathetic nervous system
Glands
34-18
19. Adrenal Glands (cont.)
• Adrenal cortex
– Outermost portion
– Secretes many hormones, but main ones are
• Aldosterone
– Stimulates body to retain sodium and water
– Important in maintaining BP
• Cortisol
– Released when stressed
– Decreases protein synthesis, resulting in slowed tissue
repair
– Decreases inflammation
34-19
20. Apply Your Knowledge
Match the following:
ANSWER:
____ Adrenal medulla
B, D
A. Cortisol
C
____ Sodium retention
B. Epinephrine
A
____ Decreases inflammation
C. Aldosterone
B, D
____ Sympathetic effects
D. Norepinephrine
____ Maintains blood pressure
C
Excellent!
____ Released during stress
A
A, C
____ Adrenal cortex
34-20
21. 34-21
Pancreas
• Located behind the
stomach
• Both exocrine gland and
endocrine gland
– Exocrine – secretes
digestive enzymes into a
duct leading to the small
intestine
– Endocrine – secretes
hormones into bloodstream
Glands
22. Pancreas (cont.)
• Islets of Langerhans secrete hormones into
bloodstream
– Alpha cells secrete glucagon
– Beta cells secrete insulin
Blood glucose
concentrations
Blood glucose
concentrations
Protein synthesis
Protein synthesis
34-22
23. Apply Your Knowledge
What are the effects of insulin and glucagon?
ANSWER: Insulin decreases blood glucose concentration and
increases protein synthesis.
Glucagon does just the opposite. It increases blood glucose
and decreases protein synthesis.
Yippee
!
34-23
24. Other Hormone-Producing
Organs
• Pineal body
• Thymus gland
– Small gland
– Located between
cerebral hemispheres
– Melatonin
– Located between
lungs
– Thymosin
• Promotes
production of
T lymphocytes
• Regulates circadian
rhythms
• May play a role in
onset of puberty
Glands
34-24
25. Other Hormone-Producing
Organs (cont.)
• The gonads
• Small intestine
– Ovaries
– Secretin
– Cholecystokinin
• Estrogen
• Progesterone
– Testes
• Heart
– Atrial natriuretic
peptide – regulates BP
• Testosterone
• Stomach
– Gastrin
• Kidneys
– Erythropoietin –
stimulates blood cell
production
34-25
Glands
27. Apply Your Knowledge
Match the following:
ANSWER:
D
___ Between lungs
A. Pineal body
A
___ Melatonin
B. Heart
G
___ Estrogen/testosterone
C. Kidneys
F
___ Gastrin
D. Thymus gland
E
___ Secretin
E. Small intestine
C
___ Erythropoietin
F. Stomach
B
___ Atrial natriuetic peptide
G. Gonads
D
___ Thymosin
E
___ Cholecystokinin
34-27
28. 34-28
The Stress Response
• Stressor
– Any stimulus that
produces stress
– Types
• Physical factors
• Psychological factors
• Positive stimuli
29. The Stress Response (cont.)
• Physiologic response to stress caused by
hormone release
– General stress syndrome
• Increased heart rate, respiratory rate, and BP
• Increase in glucose and fatty acids in blood, which
leads to weight loss
• Increase in cortisol if stress prolonged
– Decreased body repair
– Susceptibility to illness
34-29
30. Apply Your Knowledge
Match the following:
ANSWER:
___ Extreme heat
A
A. Physical stress
___ Death of friend
B
B. Psychological stress
___ Fractured leg
A
C. Positive stimulus
___ Wedding
C
___ Exam
B
___ Hearing an explosion nearby
B
___ “A” on an exam
C
___ Flu
A
___ Car stolen
B
34-30
31. 34-31
Common Diseases and Disorders
Disease/Disorder
Acromegaly
Description
Too much growth hormone produced in adults;
enlargement of bones and thickened skin
Addison’s disease Adrenal gland fails to produce enough
corticosteroids
Cretinism
Extreme form of hypothyroidism present prior
to or soon after birth
Cushing’s disease Hypercortisolism; over-production of cortisol
Diabetes insipidus Kidneys fail to reabsorb water, resulting in
excessive urination; hyposecretion of ADH
32. 34-32
Common Diseases and Disorders
(cont.)
Disease/Disorder
Diabetes mellitus
Description
Chronic disease characterized by elevated
blood glucose levels
Type I
Insulin-dependent diabetes mellitus; usually develops
in childhood
Noninsulin-dependent diabetes mellitus; primarily in
adults but increased incidence in teens
Occurs during pregnancy; usually temporary
Type II
Gestational
Dwarfism
Too little growth hormone (somatotropin)
produced during childhood
33. 34-33
Common Diseases and Disorders
(cont.)
Disease/Disorder Description
Gigantism
Too much growth hormone produced during
childhood
Goiter
Enlargement of thyroid gland, causing
swelling in neck; deficiency of iodine in diet
Grave’s disease
Hyperthyroidism; antibodies attach to thyroid
gland, causing it to produce too much thyroid
hormone
Thyroid gland produces inadequate amounts of
thyroid hormone; common in females over 50
Myxedema
34. Apply Your KnowledgeCorrect!
True or False:
ANSWER:
in an adult
___ Acromegaly develops as a result of too much growth hormone in a child.
F
T
___ In diabetes insipidus, the kidneys fail to reabsorb water.
___ Too little growth hormone in childhood results in dwarfism.
T
___ Myxedema is the result of hyperthyroidism.
F
hypothyroidism
___ Addison’s disease is the result of too little corticosteroid.
T
___ Cushing’s disease is the result of too little ACTH.
F
too much ACTH
___ Cretinism is an extreme form of hyperthyroidism present at birth.
F
hypothyroidism
34-34
35. In Summary
• The organs of the
endocrine system
secrete hormones
directly into blood and
other body fluids.
• Hormones secreted by
the endocrine system
control the functions
of other cells.
• Endocrine organs
–
–
–
–
–
–
–
–
–
34-35
Hypothalamus
Pituitary gland
Thyroid gland
Parathyroid glands
Adrenal glands
Pancreas
Pineal body
Thymus gland
Gonads, stomach small
intestine, heart,
kidneys