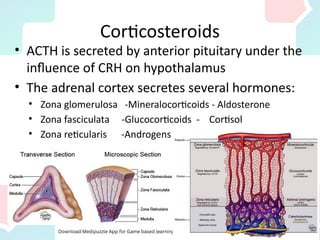
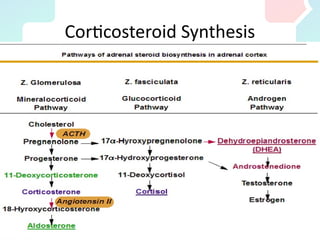
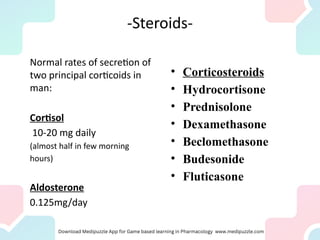
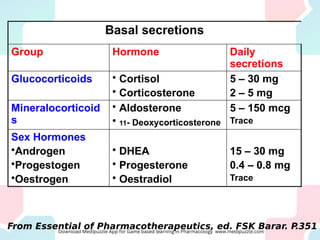
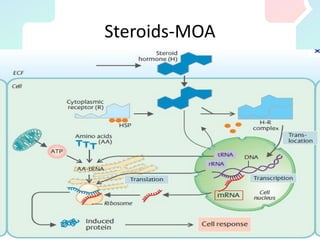
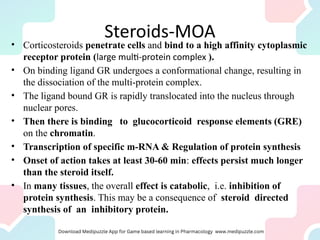
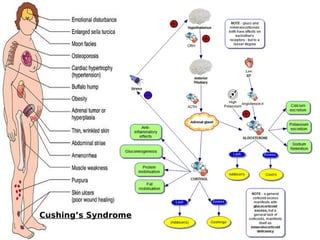
Corticosteroids, predominantly glucocorticoids like cortisol, are steroid hormones crucial for various physiological processes, including inflammation regulation and metabolism, released by the adrenal cortex. They are synthesized on demand and exert effects by binding to glucocorticoid receptors, influencing gene transcription and protein synthesis. Therapies utilizing synthetic glucocorticoids aim to manage inflammatory conditions, suppress immune responses, and ensure appropriate hormonal replacement while considering potential side effects and withdrawal protocols.
![Steroids
• Steroid: A group of compound, having a
common structure based on the steroid
nucleus.
• For examples:
– Sex hormones [androgen and estrogens],
– Hormones of the adrenal cortex [cortisone].](https://image.slidesharecdn.com/acrurdpesye06fiackbg-endo-corticosteroids-230309004849-d1eb8030/85/Endo-_CORTICOSTEROIDS-pdf-5-320.jpg)


















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)






