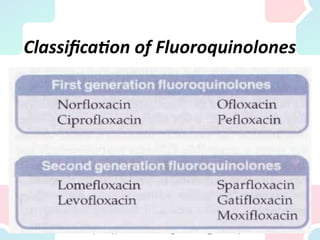
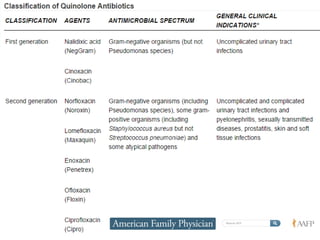
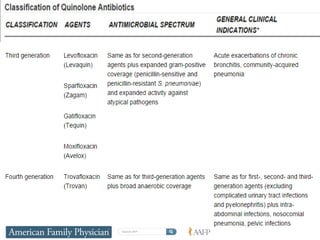
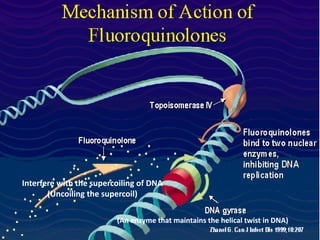
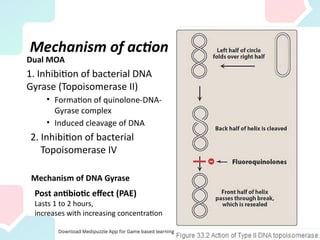
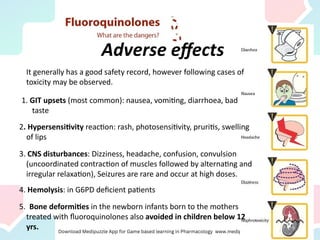
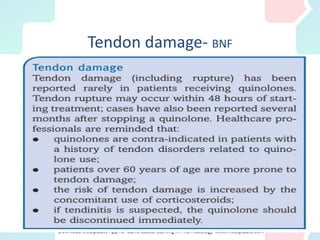
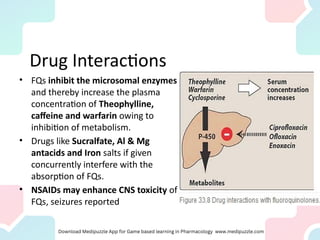
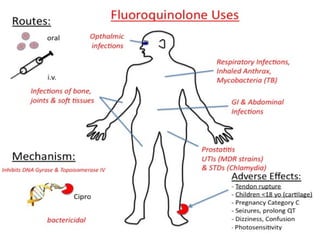
Quinolones and fluoroquinolones are synthetic antibacterial agents with a broad spectrum and different classes, including non-fluorinated and fluorinated varieties, that are primarily used for treating various bacterial infections, particularly urinary tract infections. They function by inhibiting bacterial DNA gyrase and topoisomerase, thereby preventing DNA replication, but face rising resistance among certain bacteria. Adverse effects can include gastrointestinal disturbances, hypersensitivity, CNS effects, and contraindications include pregnancy and use in children under 12 due to risk of chondrotoxicity.