
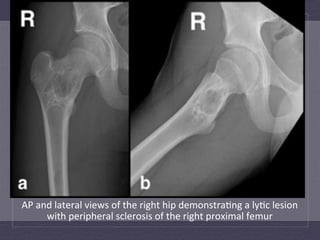
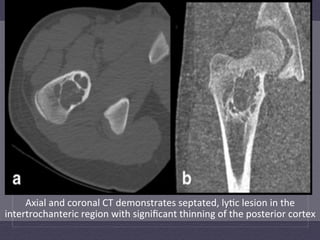
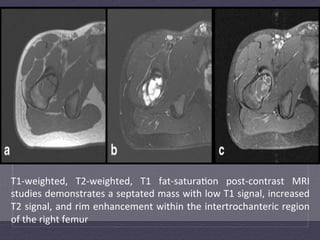
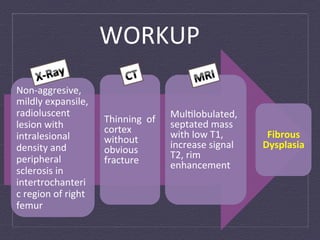
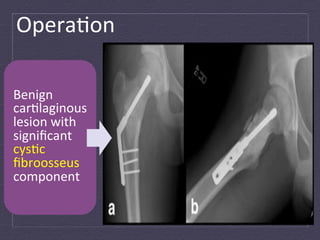
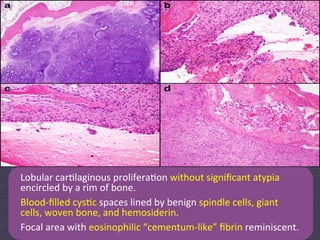








This case report describes an unusual case of an enchondroma with secondary aneurysmal bone cyst formation in the proximal femur of a 13-year-old male. Imaging showed a septated lytic lesion in the intertrochanteric region. Histology revealed lobulated cartilaginous proliferation without atypia surrounded by bone and blood-filled cystic spaces, consistent with a secondary aneurysmal bone cyst arising from the enchondroma. This is a rare occurrence, as cystic changes are not usually seen in enchondromas. The patient will need monitoring due to the higher recurrence risk of aneurysmal bone cysts compared to typical enchondromas.























































































