Download to read offline

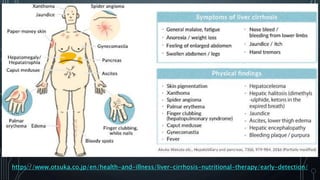
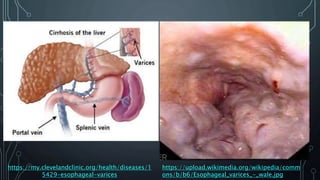








1) Variceal bleeding occurs in patients with cirrhosis and portal hypertension when enlarged veins in the esophagus or stomach (varices) rupture. 2) Management of variceal bleeding involves stabilizing the patient, performing endoscopy within 12 hours to identify varices, and administering vasoactive drugs to control bleeding along with antibiotics to prevent infection. Endoscopic variceal ligation or sclerotherapy can help stop active bleeding from varices. 3) For non-variceal upper GI bleeding, endoscopic treatment with adrenaline, coagulation, or clips is usually attempted first. Surgery may be needed for uncontrolled or recurrent bleeding after failed endoscopic attempts.























































































