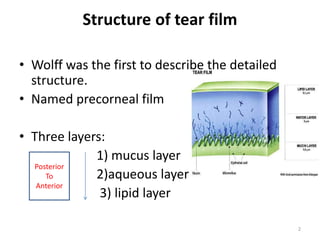
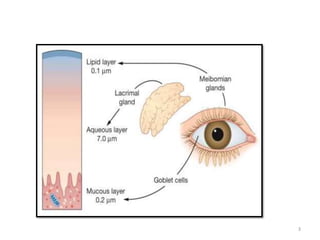
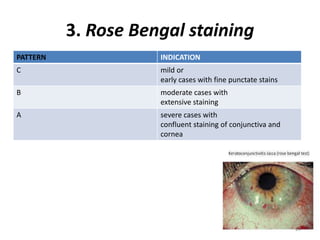
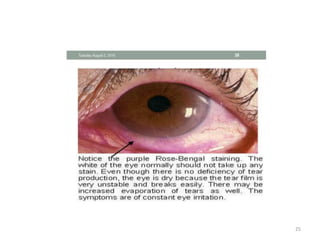
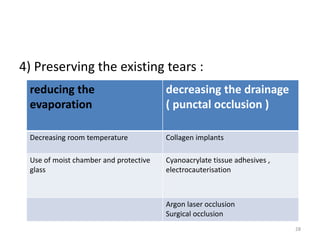
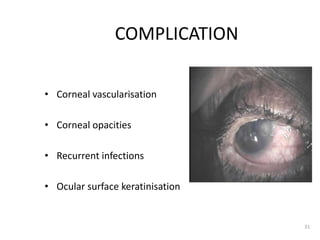
The document outlines the structure and function of the tear film, highlighting its three layers: mucus, aqueous, and lipid. It discusses dry eye conditions, their causes, clinical features, and diagnostic tests. Treatment methods for dry eye include tear substitutes, anti-inflammatory medication, and interventions to reduce tear evaporation.






































![Dry_Eye_Presentation_Final[1].pptx......](https://cdn.slidesharecdn.com/ss_thumbnails/dryeyepresentationfinal1-250516163834-f963ff70-thumbnail.jpg?width=640&height=640&fit=bounds)



























![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
