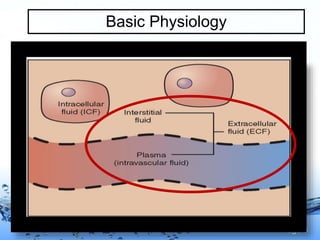
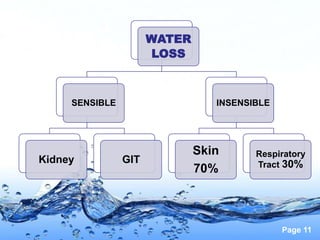
This document discusses fluid management in neonates. It covers neonatal fluid physiology, insensible water loss, factors affecting it, ways to minimize it, fluid assessment, laboratory parameters to assess fluid status, maintenance fluid requirements, and special considerations for conditions like respiratory distress syndrome, birth asphyxia, and patent ductus arteriosus. The key goals of fluid therapy in newborns are to maintain appropriate extracellular fluid volume and composition, electrolyte concentrations, and pH balance.







































![fluid_and_electrolytes[1] [Read-Only].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/fluidandelectrolytes1read-only-250903084601-61978d1f-thumbnail.jpg?width=640&height=640&fit=bounds)


























































