Downloaded 20 times


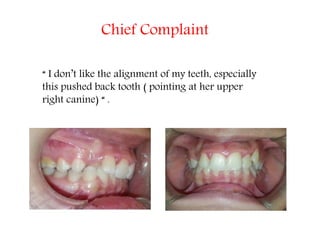







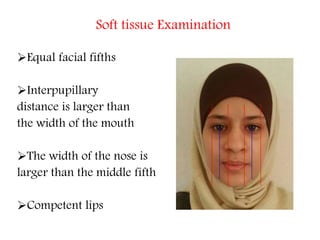


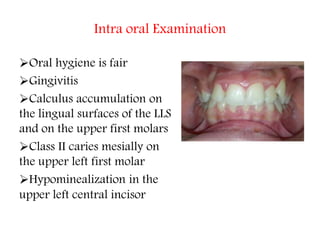


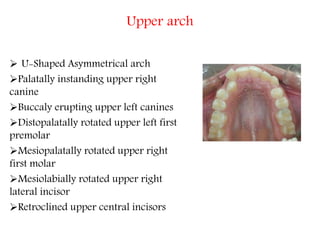
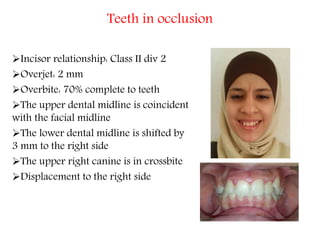
















This case presentation summarizes the orthodontic treatment of a 15-year-old female patient. The patient's chief complaint was the alignment of her teeth, particularly her palatally positioned upper right canine. Clinical examination revealed class II malocclusion, gummy smile, rotated and tipped teeth. Treatment goals were to correct the malocclusion through non-extraction therapy using fixed appliances along with headgear and bite turbos. The proposed treatment plan was to address the patient's oral hygiene, align and level the teeth to achieve class I occlusion, and provide retainers.











































































