9. Results
Mean age 59.4 ± 13.5 years
Mean duration 10 ± 7.6 years
F = 65.9%
Other 0.5% Type1
Uncertain 0.4%
4.5%
M= 34.1%
Type2 94.6%
N= 9,419
6 cases of MODY
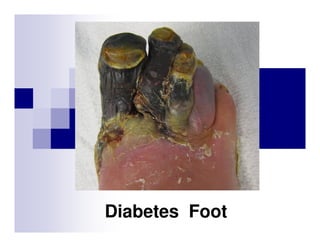
23. DM foot & Amputation
Interesting stat!!
84% from ulceration
55% from gangrene
81% from initial minor trauma
81% from faulty wound healing
36% ill-fitting shoes as a precipitating factor
24.
25. การปองกันการเกิดปัญหาเท้ าเบาหวาน
้
ผูเ้ ป็ นเบาหวานจําเป็ นต้องได้รับ การประเมินเท้าโดยละเอียด
อย่างน้อยปี ละ 1 ครัง
เพือป้ องกันการเกิดปัญหาทีเท้า ปัจจัยทีสําคัญ คือ
Good sensation
Good circulation
Standard of medical care ADA 2012
48. Ankle-Brachial Index (ABI)
Noninvasive evaluation for peripheral arterial disease
(PAD) to determine arterial stenosis.
95% sensitivity and almost 100% specific.
The ratio of systolic blood pressure of ankle to brachial.
ABI
=
ankle systolic BP
brachial systolic BP
American Diabetes Association Position Statement, Diabetes Care, Dec 2003
49. Ankle-Brachial Index (ABI)
ข้อบ่งชีในการตรวจ ABI ได้แก่
ผูป่วย DM ทีมีอายุมากกว่า 50 ปี ถ้าปกติให้ติดตามทุก 5 ปี
้
ผูป่วย DM ทีมีอายุมากกว่า 50 ปี ทีมีปัจจัยเสี ยงต่อการเกิด PAD เช่น
้
สูบบุหรี
ความดันโลหิ ตสูง
ไขมันในเลือดสูง
เป็ นเบาหวานมานานกว่า 10 ปี
ผูทีมีอาการของ PAD เช่น leg pain, claudication, diminished foot pulse,
้
ischemic foot ulcer
American Diabetes Association Position Statement, Diabetes Care, Dec 2003
50. Ankle-Brachial Index (ABI)
Diagnostic criteria for interpretation
0.91-1.30
Normal
0.70 - 0.90
Mild obstruction
0.40 – 0.69
Moderate obstruction
< 0.40
Severe obstruction
> 1.30
Poorly compressible
American Diabetes Association Position Statement, Diabetes Care, Dec 2003
51. Ankle-Brachial Index (ABI)
Follow up ABI
>0.9
: every 2-3 years
0.5-0.9
: every 3-4 months
< 0.5
: refer to vascular specialist
If still present, refer for special vascular assessment
53. Coexisting Vascular Diseases
Atherothrombosis is commonly found in
more than one arterial bed.
(CAPRIE study, n = 19,185)
70
CAD
7.4%
24.7%
29.9%
3.3%
11.8%
3.8%
Coexistent Disease (%)
60
CVD
50
CAD
PAD
CVD
68
56
40
42
30
20
32
28
26
10
0
19.2%
PAD
Coexistent
Stroke
Lancet. 1996;348:1329–39
Coexistent
PAD
Coexistent
CAD
Ness J. et al. J Am Geriatr Soc. 1999;47:1255-1256
CVD: Cerebrovascular Disease, CAD: Coronary Arterial Disease, PAD: Peripheral Arterial Disease
54. 5-Year Natural History of PAD
“Complain of their legs butpatients with
100 die
100 patients
with asymptomatic
atypical leg pain
PAD from their Hearts & Brains”
Verstrate
Local Events
Worsening claudication
25 patients
100 patients
diagnosed with
claudication
Surgical revascularization
10 patients
Major amputation
2 patients
Dormandy. Hosp Update 1991;April:314-318;
Dormandy. Rev Prat 1995;45:32-45.
Systemic Events
10 to 20 non-fatal MIs or
strokes
PLUS
30 Deaths:
• CHD
15
• Other cardiovascular
and cerebrovascular 5
• Noncardiovascular
10
55. 5-yr Mortality Rates for PAD vs Common Malignancies
85
90
Patients (%)
80
70
60
50
38
40
28
30
20
14
16
10
0
Breast Hodgkin's
Cancer
Disease
PAD
American Cancer Society. Cancer Facts and Figures 2003
Belch JJF et al. Arch Intern Med 2003;163:884
Colon and Lung
Rectal
Cancer
Cancer
56. PAD Diagnosis: Physical Exam
u
Trophic Signs
Skin atrophy, thickened nails, hair loss,
dependent rubor
Ulceration, gangrene
u
Pulse exam
May miss more than 50%
u
Elevation and dependency test
Criqui M, et al. Circulation, 1985: 71; 516-521
57. PAD Diagnosis: History
u
Use of the history alone to detect peripheral
arterial disease will result in missing up to 90
percent of cases.
u
Asymptomatic patients with abnormal ABI have
50% increased risk of cardiovascular
complications
Hirsch AT, et al. JAMA 2001; 286: 1317
Hooi JD, et al. J Clin Epidem 2004; 57:294
59. ACC/AHA 2011 practice Guidelines for the Management of
Patients With Peripheral Arterial Disease
(Lower Extremity, Renal, Mesenteric, and Abdominal Aortic)
I IIa IIb III
B
Anti-platelet therapy is indicated to
reduce the risks of MI, stroke and
vascular death in individuals with
symptomatic PAD (Class I level A)
Aspirin 75-325 mg OD
(A B)
Clopidogrel 75 mg OD (B)
60. ACC/AHA 2011 practice Guidelines for the Management of
Patients With Peripheral Arterial Disease
(Lower Extremity, Renal, Mesenteric, and Abdominal Aortic)
I IIa IIb III
Intermittent Claudication
A
Cilostazol 100 mg BID
• Effective
• Increase walking distance
• Avoid in patients with heart
failure
61. ACC/AHA 2011 practice Guidelines for the Management of
Patients With Pheripheral Arterial Disease
(Lower Extremity, Renal, Mesenteric, and Abdominal Aortic)
I IIa IIb III
Intermittent Claudication
Pentoxyfylline 400 mg TID
A
• Second-line alternative to Cilostazol
(statistical benefit)
C
• Clinical effectiveness not well
established
62. Treatment of PAD
PAD
Assess cardiovascular
risk factors
Risk- factor modification
Smoking cessation
LDL cholesterol <100 mg/dl
Glycosylated hemoglobin <7.0%
Blood pressure <130/85 mm Hg
ACEI
Antiplatelet therapy
Aspirin or clopidogrel
ACC/AHA PAD guidelines 2006
Assess severity of claudication
Critical leg ischemia
Therapy for claudication
Supervised exercise
Cilostazol
Symptoms
improve
Continue
Symptoms
worsen
Localize the lesion
Duplex ultrasonography
MRA, CTA
Conventional angiography
Revascularization
Angioplasty
Bypass surgery
64. Neuropathic Ulcer
Painless
Occurs over bony prominences
Under metatarsal heads
Under big toe
Tip of toes
Dorsum of interphalangeal joints
Heel
Surrounded by callus
65. Ischemic Ulcer
Painful
Situated on the edge of the
foot or toes due to poor
circulation
Purple or black in appearance
due to poor blood supply
Not surrounded by callus
66. Findings
Normal foot
Sensory neuropathy
Sensory neuropathy/
deformities/ vascular
insufficiency
Sensory neuropathy/
previous foot
ulcer/amputation
Risk of ulcer
development
Frequency of
foot evaluation
Annually
1.7-fold
12.1-fold
36.4-fold
Every 3-4months
Every 2-3months
Every 1-2months