Rheumatoid arthritis
•
0 likes•319 views

Rheumatoid arthritis easy summary and practical point for GP

Recommended
More Related Content
Similar to Rheumatoid arthritis
Similar to Rheumatoid arthritis (20)
Rheumatoid arthritis
- 1. INT. TEERAPHAN KHAMJAROEN KCHOSP AUG 2018 Ref. :Essential of clinical Rheumatology 2017, CPG Thai 2557
- 2. causes 1. Hereditary : FHx of RA increased risk for 3 – 5 times, HLA-DR4 genes (Chr 6, MHC), Allele HLA-DRB1*0405 in Eastern Asia include Thailand (increase risk 3.84x) 2. Epigenetics (กระบวนการเหนือพันธุกรรม) : การปป.ของ gene ที่ถ่ายทอดทางพันธุกรรม โดยไม่มีการปป.ของลาดับ หรือตน.ของ DNA มีผลต่อ DNA methylation, microRNA 3. Environment: • Smoking – ชายที่มี RF+ และสูบบุหรี่จะมีโอกาสเป็น RA มากกว่าอีกกลุ่ม 2x และในหญิงจะมีความเสี่ยงมากกว่า 1.3x , smoking จะ การสร้าง Ab ต่อ citrullinated peptide ACPA, เพิ่ม oxidative stress, เพิ่ม apoptosis, เพิ่ม cytokine และเพิ่ม severity ของโรค RA มากกว่าคนที่ไม่สูบ • Infection – Virus (EBV, Parvovirus B19, Rubella, CMV, HSV, Retrovirus), Bacteria (Chlamydia, Mycloplasma, Proteus mirabilis, E.coli, Porphyromonas gingialis <ก่อให้เกิด periodontal dz>) เชื้อพวกนี้จะมี molecular mimicry โดยทีส่วน amino QKRAA เรียงตัวเหมือนที่อยู่บนยีน HLA-DRB1 กระตุ้นให้ข้ออักเสบ 4. Hormone: F > M : 2x – 3x , elder > younger, peak 45 – 49 yrs (postmenopause), โรค สงบในช่วง E และ P สูง, มีรายงานว่าการใช้ OCP ช่วยป้ องกัน RA ได้
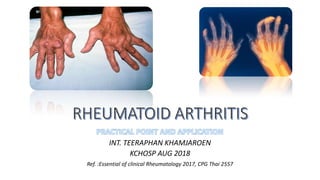
- 3. Clinical S&S • “เช้า-3-เท่า-มือ-ตุ่ม-ตอย-ฟิล์ม” • Symmetrical, M/C small jt. • Morning jt. Stiffness > 1 hr • Flexion contracture • Ulnar deviation • Swan neck deformity • Boutonniere deformity • Extensor tendon rupture • Joint ankylosis (Late) • Cock up toe deformity : M/C, extensor surface • : keratoconjunctivitis sicca (15-20%) ถ้ามี xerosomia (ปากแห้ง น้าลายน้อย) ด้วย = Sjoren’s syndrome ซึ่งจัดเป็น 2o Sjoren ในกลุ่มนี้, Episcleritis, scleromalacia perforans : ACD (75%), IDA (15%), Megaloblastic anemia ในคนที่ได้ MTX, Thrombocytosis, eosinophilia ใน ระยะกาเริบ, Felty’s syndrome (1%) พบใน chronic RA มี neutropenia < 1500, thrombocytopenia, splenomegaly มีกมี RN, vasculitis, chronic wound ที่ขา เพิ่ม risk infxn และสัมพันธ์กับ HLA-DR4, lymphadenopathy ใกล้บริเวณข้อที่อักเสบ, paraproteinemia • : Pleuritis, Interstitial pneumonitis (ILD) เป็น UIP หรือ NSIP ก็ได้, pulmonary nodule, PHT (30%) : pericarditis, pericardial effusion (30%), atherosclerosis • : rare, มักพบในคนไข้ที่ได้ยา gold salt, penicillamine ทา ให้เกิด MN, ในกลุ่มที่ได้ NSAIDs อาจมี AIN, amyloidosis, papillary necrosis : พบได้น้อย แต่พบได้หลากหลายแบบ : พบได้บ่อย โดยเฉพาะใน end-stage dz • : บริเวณรอบข้อและพบ muscle atrophy, steroid myopathy Film: marginal erosion, joint space narrowing, juxta-articular osteopenia, malalignment, joint subluxation
- 4. Boutonniere deformity Swan neck deformity Ulnar deviation Rheumatoid nodule
- 6. ACR-EULAR 2010: Se 58-85%, Sp 44-89% Se. ดีกว่า จึงนิยมกว่า และ Rx ได้เร็วกว่า ทาให้ประสิทธิภาพในการรักษาดีกว่า
- 9. : - เป็น TOC ให้ใช้ สัปดาห์ละครั้ง, ออกฤทธิ์ที่ 6-8 wk ควรให้ folic ร่วม 1-5 mg/d เพื่อลด SE, ห้ามในขณะ infxn, Pregnancy, Lactation - แบ่งให้ bid มี GI SE ค่อนข้างมากจึงควรให้ folic ร่วม, peak ที่ 2-3 mo., ห้ามให้ในคนที่แพ้ Sulfa, ASA,G6PDD, Lactation แต่ให้ใน pregnancy ได้ - effectiveness ต่าสุดในกลุ่ม มักใช้เสริม MTX, peak ที่ 2-3 mo., ยาจะสะสมที่ skin และ macula ทาให้เกิด Bull’s eye maculopathy ตามัว หรือบอดได้ irreversible ใช้ได้ใน pregnancy, Renal/Liver dz แต่ควรปรับ dose, ไม่ควรใช้ใน Lactation
- 10. F/U assessment • Clinical • SE of Tx • Pain and Severity of dz: PAS, PAS II, RAPID3, CDAI, SDAI, DAS28 ,DAS28-ESR, DAS28-CRP แต่ที่แนะนาให้ใช้คือ ACR/EULAR Boolean หรือ index base definition: • โรคสงบ คือ จานวนข้อกดเจ็บ ≤ 1 ข้อ, จานวนข้อบวม ≤ 1 ข้อ, CRP < 1 mg/dL และ • PGA < 1 ใน visual analog scale : โรคสงบ คือ SDAI ≤ 3.3
- 11. : เพื่อบรรเทาอาการปวด และลด joint stiffness เพิ่ม ROM และ muscle strengthening - การแช่น้าอุ่น พาราฟิน - คลื่น ultrasound - QD exercise
- 12. Conclusion: Rheumatoid arthritis Chronic polyarthritis: อาการและตาแหน่งเข้าได้กับ RA Criteria dx: ACR/EULAR 2010 ACR 1987 RF, ACPA ESR or CRP Film hands or feet DDx อย่างอื่น: Gout, Septic arthritis, CNT dz อื่นๆ -Uric, CBC, UA, ANA, HBsAg, AntiHCV, AntiHIV -Synovial fluid profiles Definite Treatment modality Pain control: -NSAIDs -Tramol -Tramol+Para Pred 7.5 mg/d เมื่อมีข้อบ่งชี้: -อาการรุนแรงจนทากิจวัตรประจาวัน/ทางาน ไม่ได้ -ไม่ตอบสนองต่อ NSAIDs -มีข้อห้ามในการให้ NSAIDs เช่น โรคไต, โรคตับ DMARDs: MTX, SSZ, HCQ, CQ Start Max ปรับทีละ ปรับยาทุก MTX (mg/wk) ให้ยา wkly 5 – 7.5 10 2.5 4 – 12 wk SSZ (mg/d) 1000 2000 500 4 – 12 wk CQ (mg/d) 125 – 250 250 125 12 wk HCQ (mg/d) 200 400 200 12 wk PT มี poor prognostic factors?: -ข้อบวมหลายข้อ -ROM ของข้อจากัดมากๆ -มี extra-articular sx : rheumatoid nodule, vasculitis -RF หรือ ACPA +ve -ESR หรือ CRP สูง -มี erosion,osteopenia จาก film ใช้ combinationติดตามอาการ และ SE ของยา ทุก 1 – 3 เดือน Remission นานอย่างน้อย 6 เดือน: SDAI ≤3.3 หรือ PGA < 1 และมีข้อกดเจ็บและบวมไม่เกิน 1 ข้อและ CRP < 1 (ถ้าไม่มี CRP ให้ใช้ ESR แทน) ให้ลดยา มีข้อบ่งชี้ในการ refer?: -ไม่แน่ใจ dx -มี comp จาก dz หรือ extra-articular sx ที่รุนแรง -multiple co-morbidity -ไม่ตอบสนองต่อ high dose DMARD นานอย่างน้อย 3 – 6 เดือน -off Pred ไม่ได้ภายใน 6 -12 เดือน -มี comp จากการรักษา -Pregnancy or Lactation หลังเริ่มยา ก่อนเริ่มยา ไม่เข้าเกณฑ์