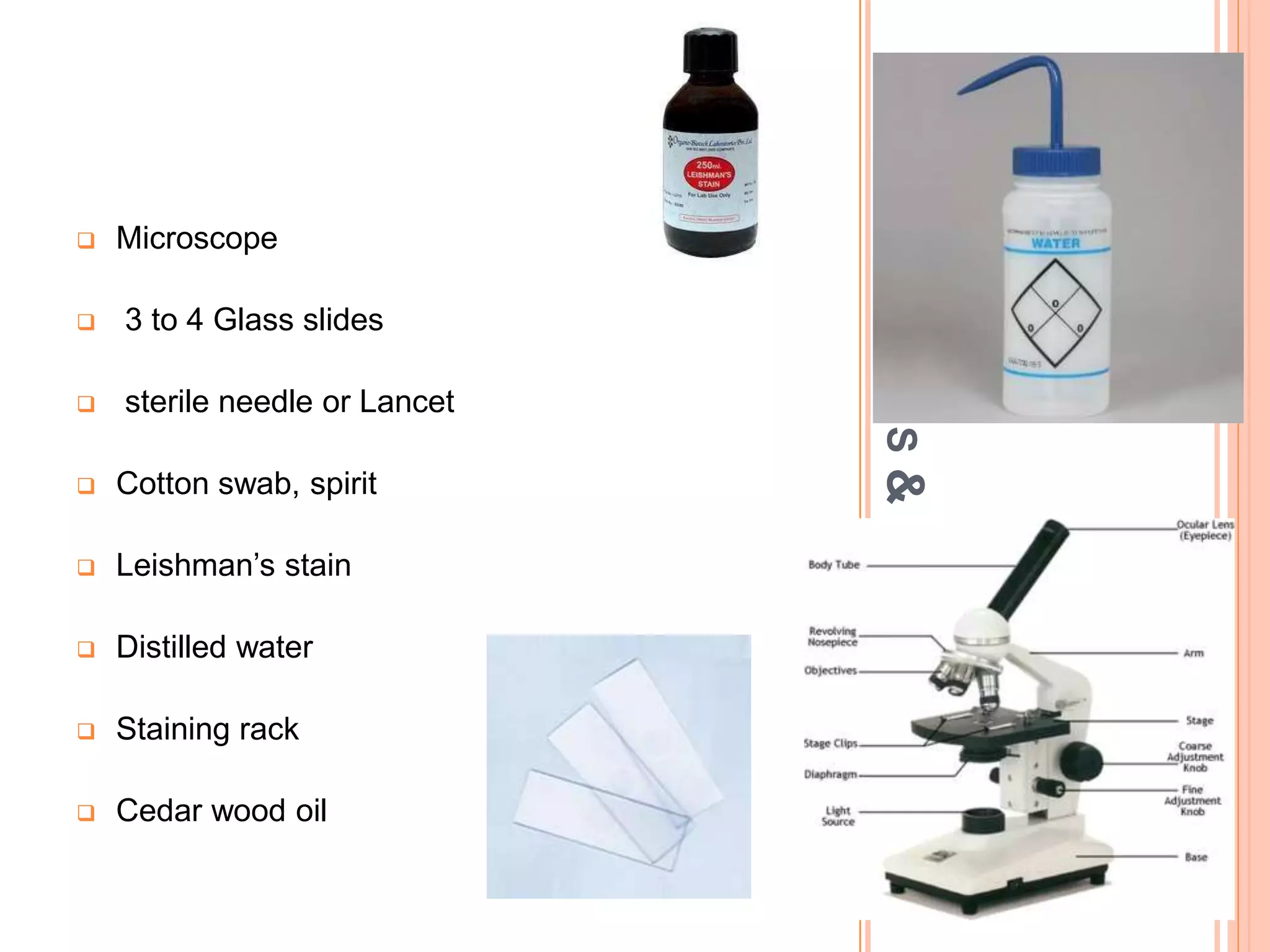
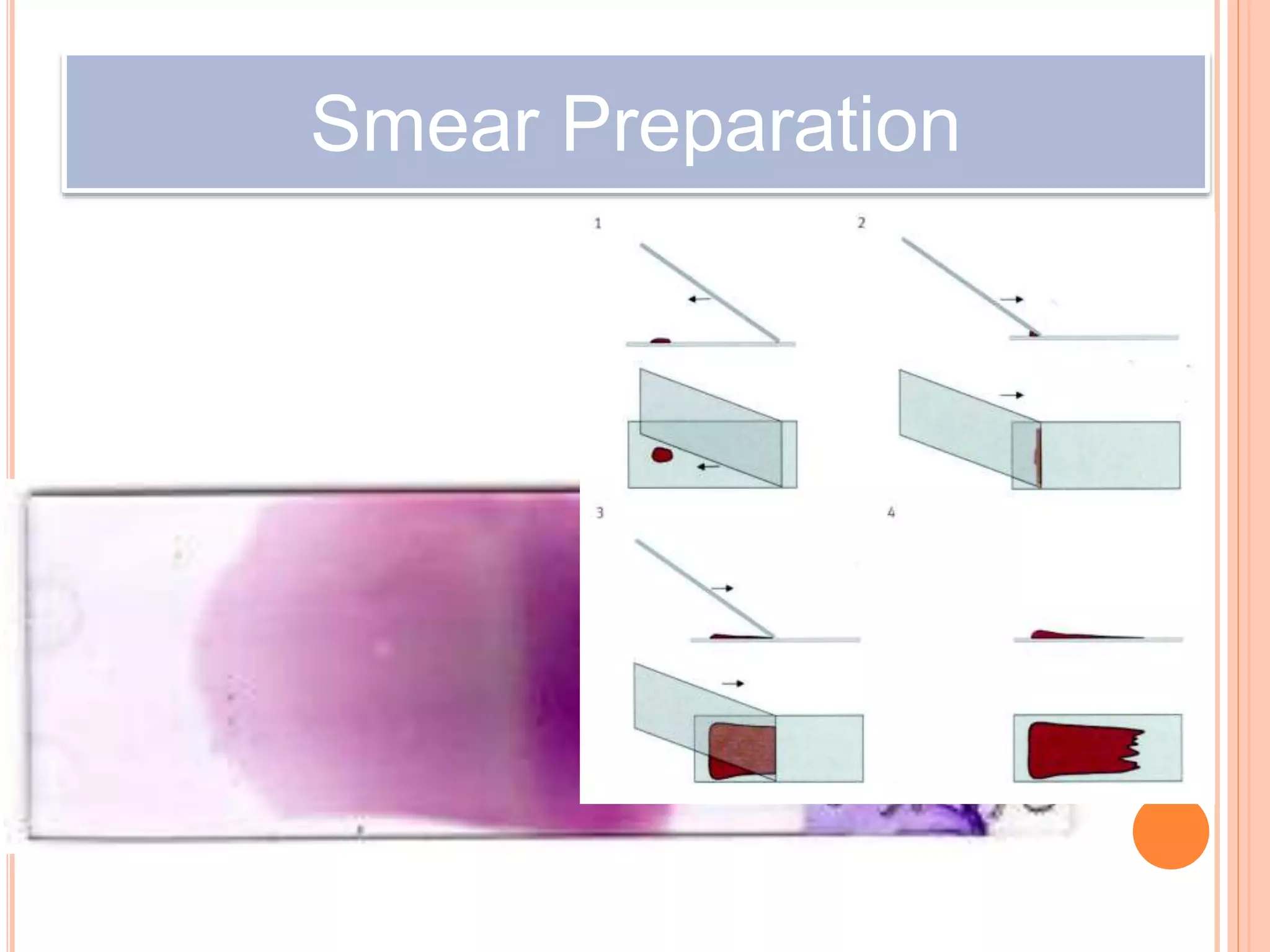
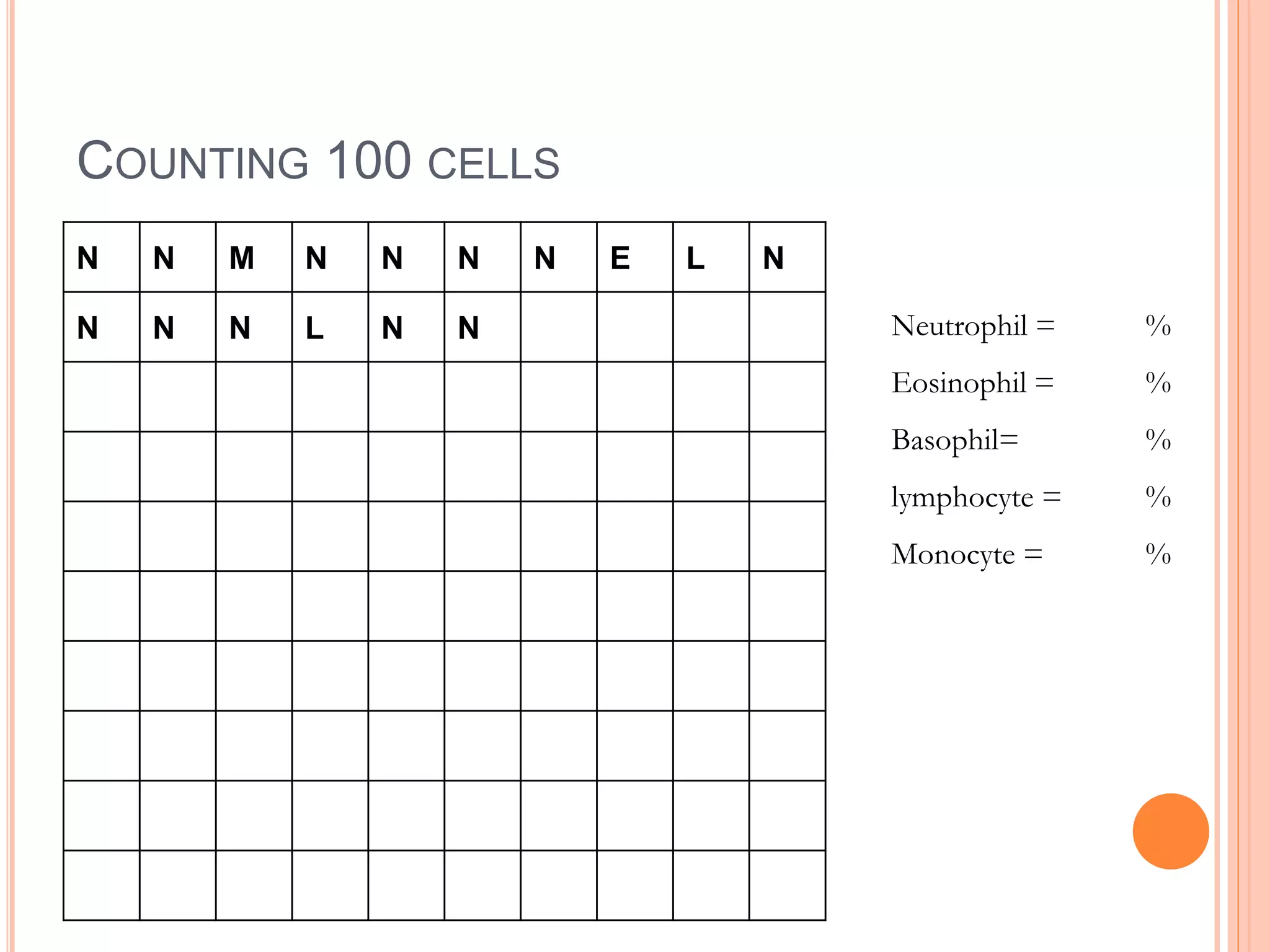
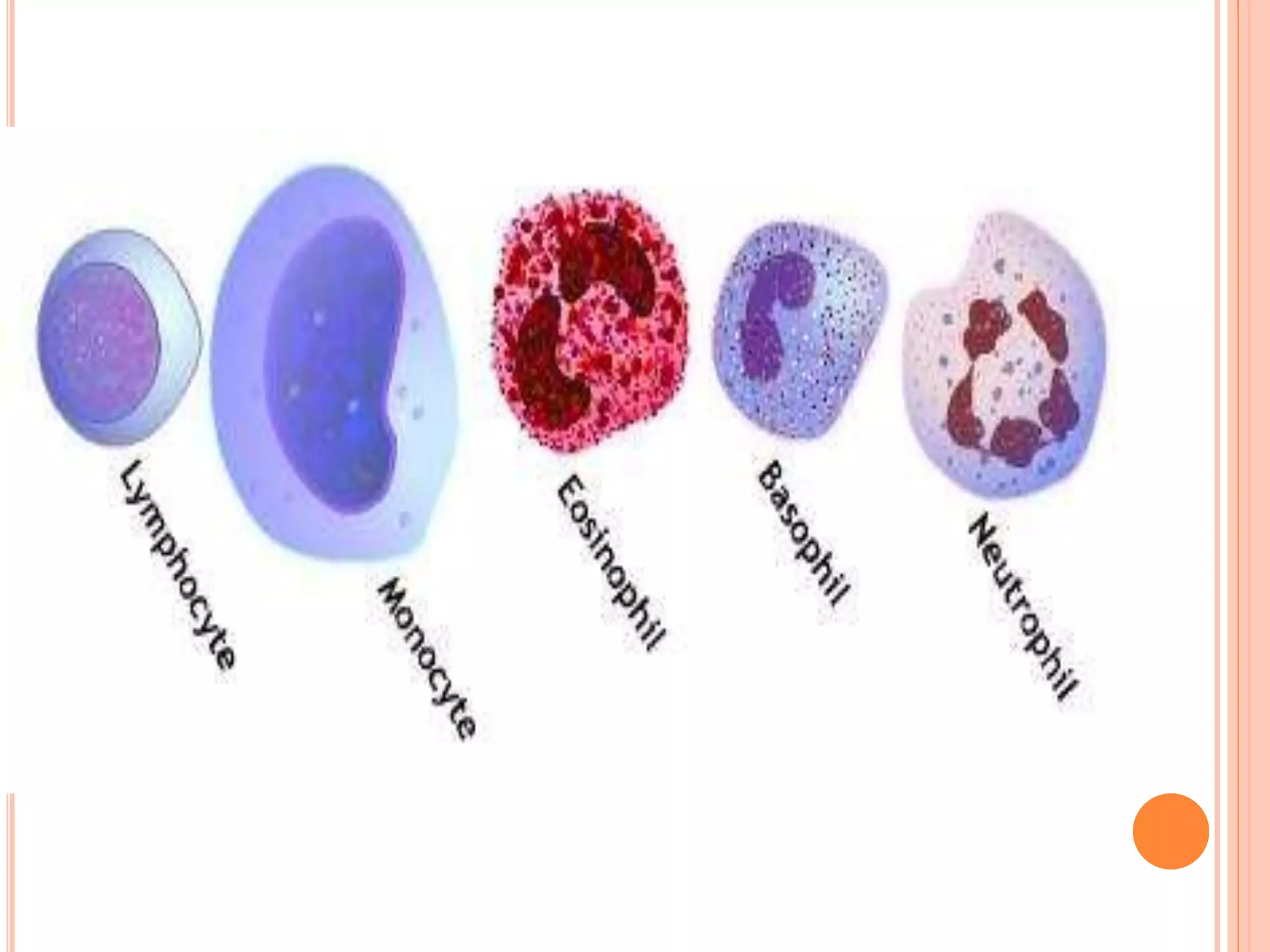
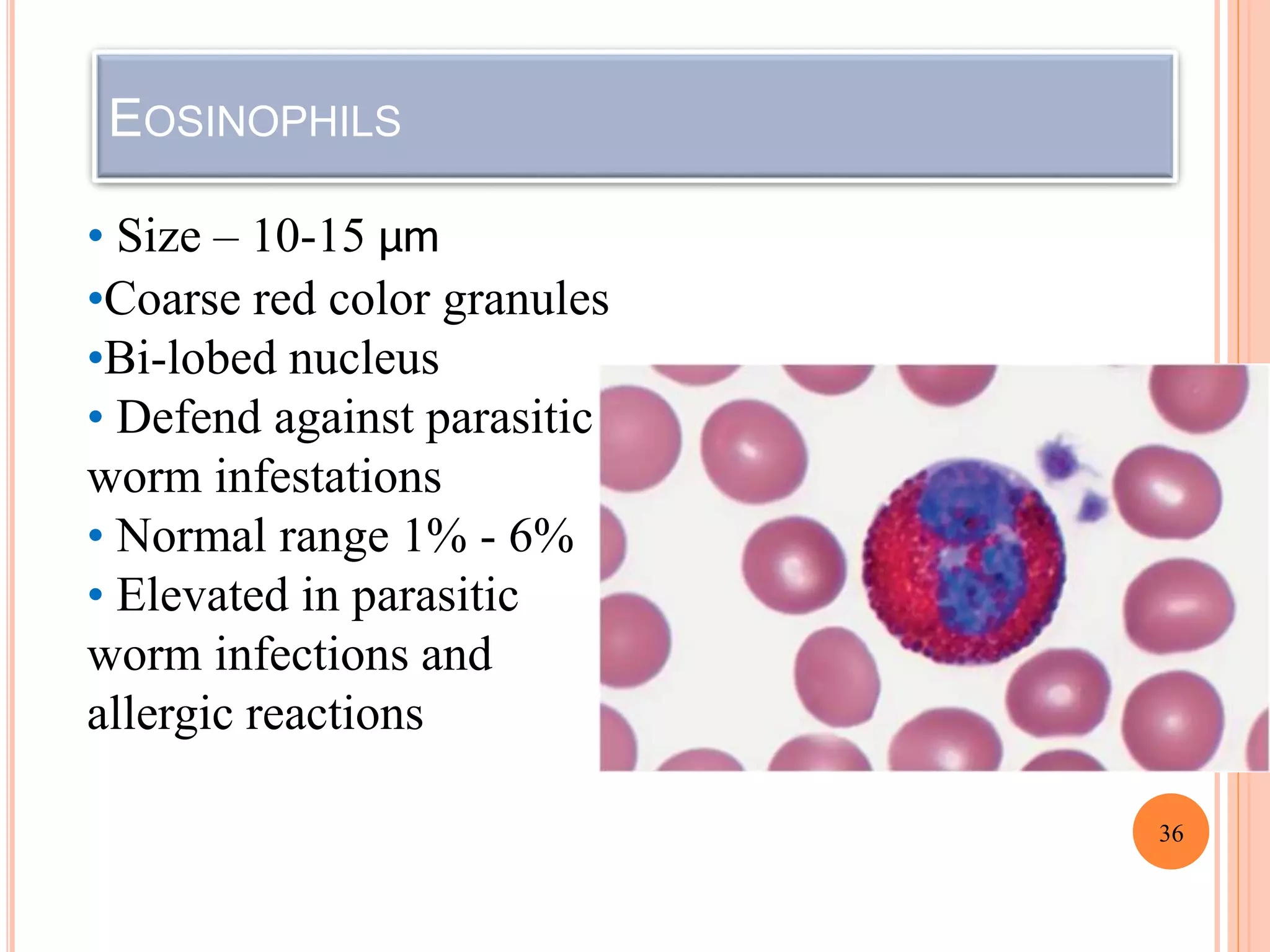
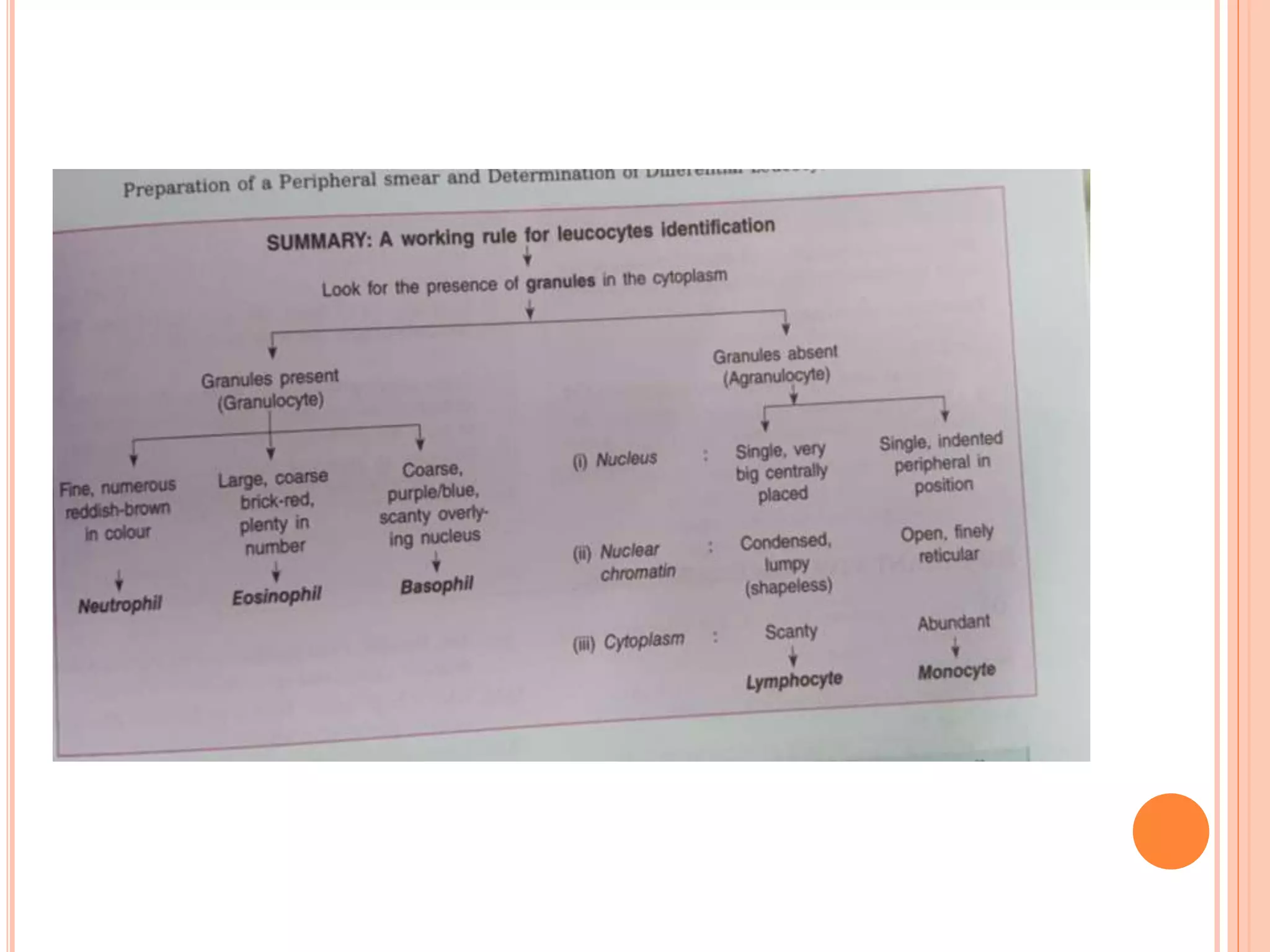
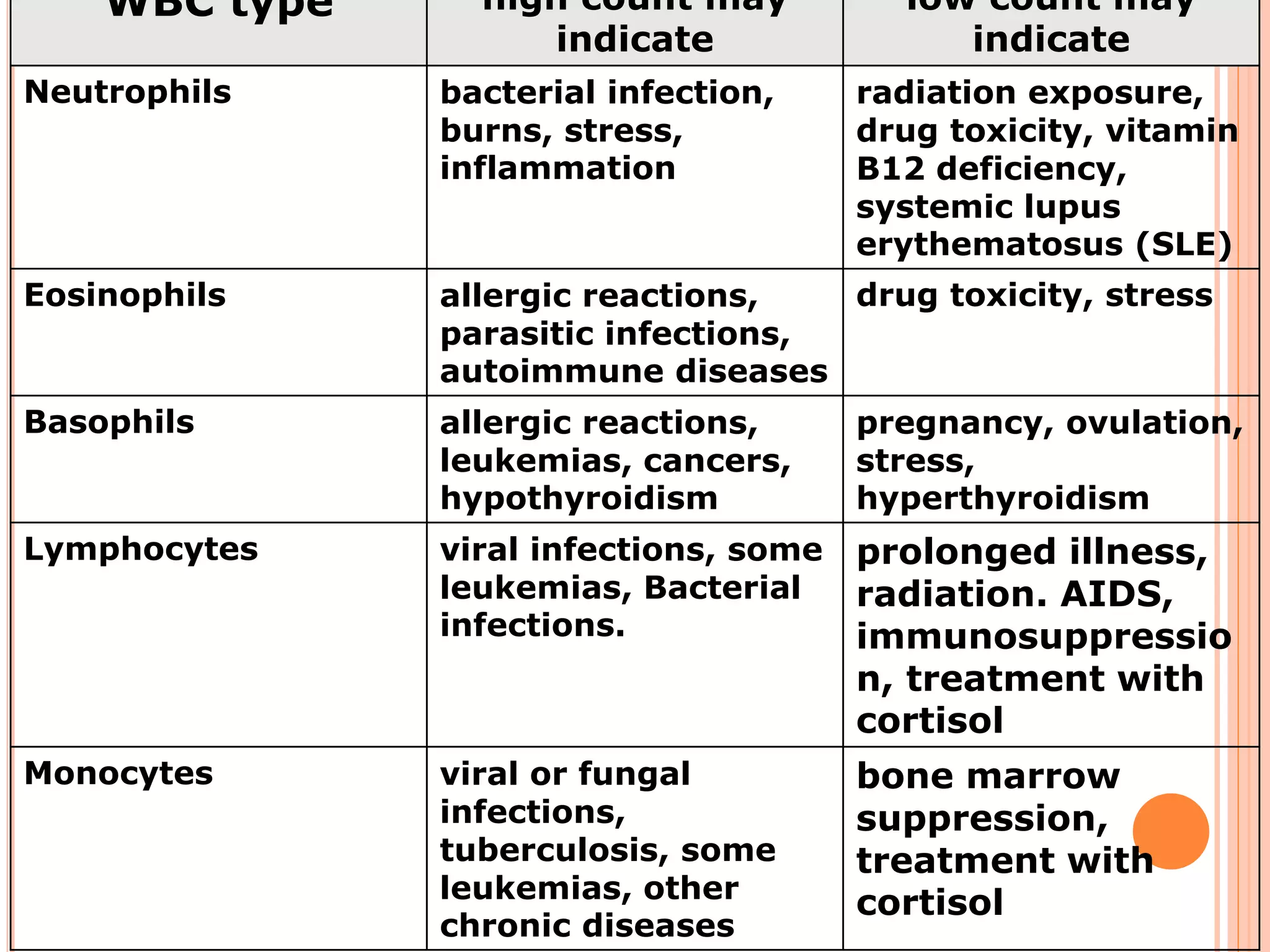
The document describes the process of performing a differential leukocyte count (DLC) from a blood smear. It involves preparing a blood smear, staining it with Leishman's stain, then examining it under a microscope. The key steps are identifying and counting 100 white blood cells to determine the percentage of each type present - neutrophils, lymphocytes, monocytes, eosinophils and basophils. An increased percentage of a particular type can indicate different diseases or infections. The DLC provides information about the immune status and helps diagnose conditions affecting white blood cell levels.



























































![Peripheral blood smear [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/peripheralbloodsmearautosaved-201029200454-thumbnail.jpg?width=640&height=640&fit=bounds)












































![Understanding Parkinson’s Disease: Causes, Symptoms, and Treatment [2025]](https://cdn.slidesharecdn.com/ss_thumbnails/understandingparkinson-251208102525-80ba3223-thumbnail.jpg?width=640&height=640&fit=bounds)






