Download to read offline






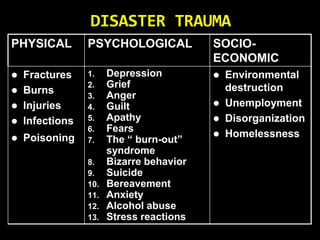













1. The document discusses disaster management and defines disasters as events that cause significant damage and loss of life, requiring an extraordinary response. 2. Disasters are classified based on their origin as natural (e.g. floods, earthquakes) or human-induced (e.g. industrial accidents, terrorism). They can also be sudden or slow-onset. 3. Disaster nursing aims to meet survivors' basic needs and promote health, using principles like rapid assessment and triage to prioritize life-saving care.
















































































