Downloaded 16 times

![¿Qué es vía aérea difícil?
1. Difficult facemask or supraglottic airway (SGA) ventilation
(e.g. , laryngeal mask airway [LMA]): It is not possible for the
anesthesiologist to provide adequate ventilation
2. SGA placement requires multiple attempts, in the presence
or absence of tracheal pathology.
3. It is not possible to visualize any portion of the vocal cords
after multiple attempts at conventional laryngoscopy.
4. Difficult tracheal intubation: Tracheal intubation requires
multiple attempts, in the presence or absence of tracheal
pathology.
5. Failed intubation: Placement of the endotracheal tube fails
after multiple attempts.
Apfelbaum JL, Hagberg CA, Caplan RA, et al; American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Practice guidelines for
management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology.
2013 Feb;118(2):251-70.](https://image.slidesharecdn.com/viaaereadificil-180212202239/85/Difficult-airway-2-320.jpg)
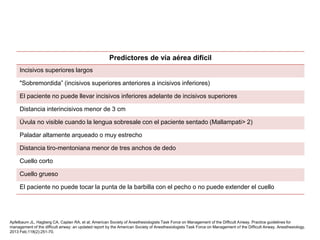
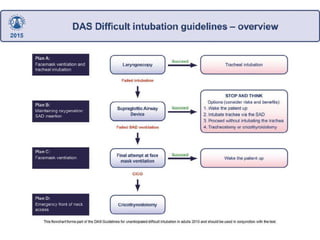








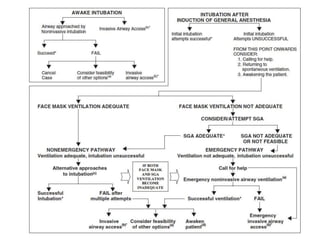

The document discusses the management of difficult airways in anesthesiology, defining what constitutes a difficult airway and outlining key predictors and strategies for intervention. It emphasizes the importance of having backup plans, limiting attempts at airway intervention, and effective communication within medical teams to mitigate risks. Additionally, it presents various techniques and guidelines for handling situations of failed intubation and ensuring patient safety.



































![Anesthesia_for_Airway_management_and_Difficult_airway_Algorithmss[1][1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/anesthesiaforairwaymanagementanddifficultairwayalgorithmss11-250722203414-f94048f1-thumbnail.jpg?width=640&height=640&fit=bounds)














![Consideraciones anestésicas en cirugía de aorta torácica [Autoguardado].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/consideracionesanestesicasencirugiadeaortatoracicaautoguardado-250127204623-d3feedba-thumbnail.jpg?width=640&height=640&fit=bounds)




































