Importance of airwaymanagement
• Holds the top priority in the PRACTICE OF MEDICINE.
• No organ system can be resuscitated before securing the airway.
• Inability to manage airway can be catastrophic to the patient.
3.
Difficult and failedairway management accounts for 2.3% to 16.6% of anaesthetic
deaths, tracheal intubation for 17% of the respiratory related injuries and up to 28%
of all anaesthetic related deaths are secondary to the inability to mask ventilate or
intubate; thence the following steps become essential to favourably affect outcome:
1. Thorough airway history and physical examination.
2. Assessment of the airway to predict
• Difficult airway: can be predicted by thorough history and if there is presence of
Congenital anomalies like Pierre Robbin or Down syndrome.
• Difficult bag and mask ventilation: Indices like OBESE, BONES helps in prediction.
• Difficult laryngoscopy and intubation: Group indices like LEMON, WILSON etc
could be used .
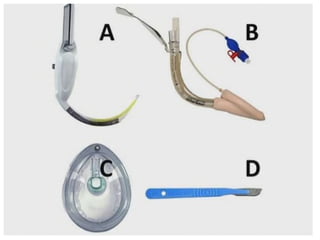
3. Preinduction formation of a management plan which includes supraglottic
ventilation (eg:supraglottic airway)
4. Aspiration risk assessment
5. Estimation of the risk of failed airway manoeuvres
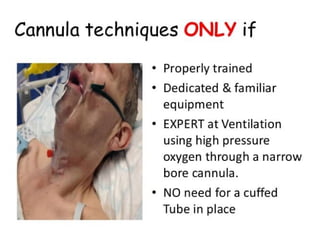
SAFE AIRWAY MANAGEMENT
5.
THE DIFFICULT AIRWAY:
•Difficult mask ventilation
• Difficult laryngoscopy
• Difficult intubation
The ASA defined difficult airway as “The clinical situation in which a conventionally
trained anaesthesiologist experiences difficulty with mask ventilation, difficulty with
tracheal intubation or both”.
•Difficult mask ventilation
It is not possible for the unassisted anaesthesiologist to maintain oxygen saturation
more than 90% using 100%oxygen and positive pressure mask ventilation in a patient
whose oxygen saturation was more than 90% before anaesthetic intervention and or
it is not possible for the unassisted anaesthesiologist to prevent or reverse the signs
of inadequate ventilation during positive mask ventilation.
6.
•Difficult laryngoscopy
“It isnot possible to visualise any portion of vocal cords with conventional
laryngoscopy”
•Difficult intubation (ASA task force)
Proper insertion of the tracheal tube with conventional laryngoscopy requires
more than three attempts or more than 10 minutes.
• Difficult intubation(Canadian Airway Focus Group)
An experienced laryngoscopist, using direct laryngoscopy, requires:
⮚>2 attempts with same blade
⮚A change in blade or an adjunct to direct laryngoscope (i.e bougie) or
⮚Use of alternative device or technique following failed intubation with direct
laryngoscopy
7.
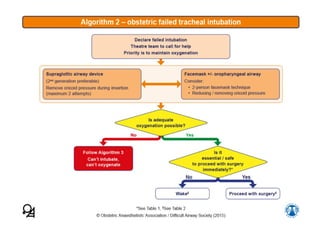
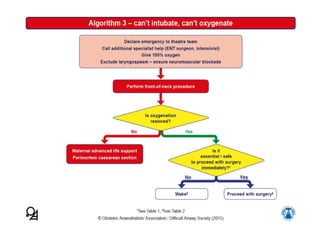
COMPLETE VENTILATION FAILURE
Previouslythe situation where tracheal intubation, face mask and
SAD failed was labelled as ‘Cannot ventilate or Cannot intubate or
Cannot oxygenate’. We define complete ventilation failure (CVF) is
a situation where intubation, ventilation using SAD have all failed
after giving the best attempt even if oxygenation may be
mainatinned.
8.
The purpose behindthis presentation is to make one aware
about some of the important algorithmic approaches to prevent
the adverse outcomes associated with difficult airway(which
include but are not limited to) damage to teeth, airway trauma,
unnecessary surgical airway, cardiopulmonary arrest, brain injury
and death.
‣ In today’s presentation we shall be dealing with the difficult
airway algorithms given by :
• AIDAA: All India Difficult Airway Association, a non profit
voluntary organization that exists for the promotion of airway
management in the country. The society was found in 2010 in
Mangalore.
• DAS: Difficult Airway society, a U.K. based medical speciaist
society
9.
AIDAA GUIDELINES
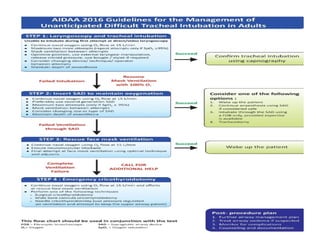
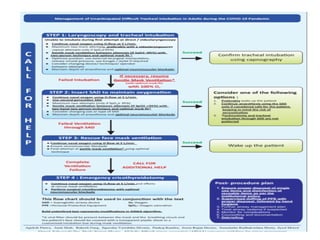
The AllIndia Difficult Airway Association (AIDAA) guidelines for
management of the unanticipated difficult airway in adults provide a
structured, stepwise approach to manage unanticipated difficulty during
tracheal intubation in adults. They have been developed based on the
available evidence; wherever robust evidence was lacking, or to suit the
needs and situation in India, recommendations were arrived at by
consensus opinion of airway experts, incorporating the responses to a
questionnaire sent to members of the AIDAA and the Indian Society of
Anaesthesiologists.
10.
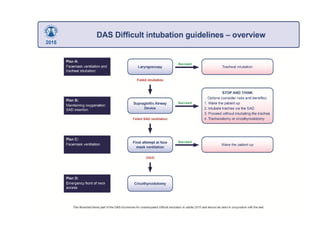
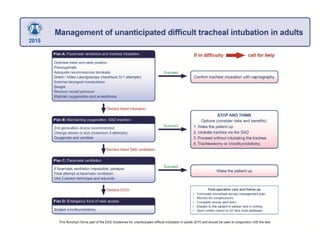
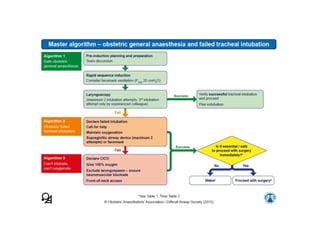
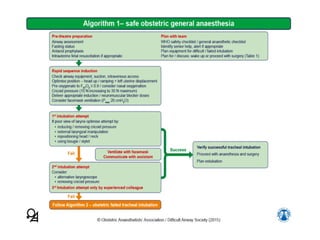
DAS Guidelines
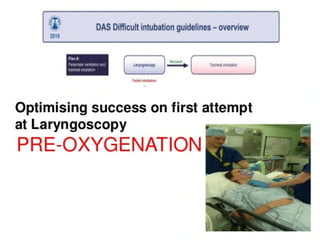
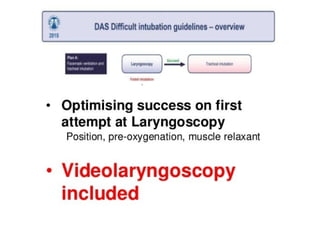
The DASflow-charts are based on a series of plans. The philosophy of having a series
of plans is well established in airway management as no single technique is always
effective.. Effective airway management requires careful planning so that back up plans
(plan B, C, D) can be executed when the primary technique (plan A) fails. This
philosophy forms the basis of the DAS guidelines. It is hoped that anaesthetists will
always make back up plans before performing primary techniques so that adequate
expertise, equipment and assistance are available.
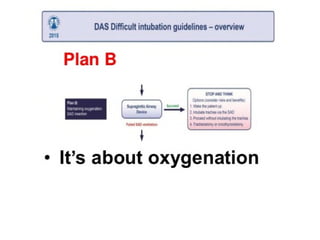
Two other principles are particularly important. Maintenance of oxygenation takes
priority over everything else during the execution of each plan. Anaesthetists should
seek the best assistance available as soon as difficulty with laryngoscopy is
experienced.
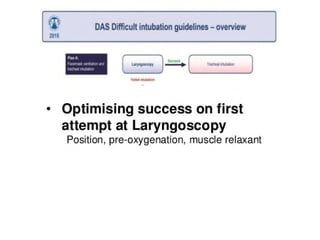
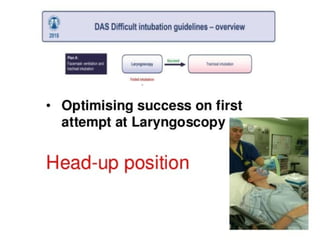
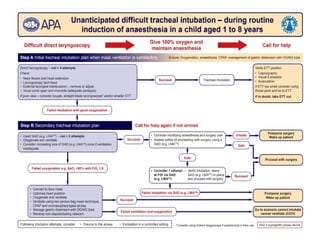
It includes optimumpre-oxygenation and nasal insufflation of 15 L/min oxygen during
apnoea in all patients, and calling for help if the initial attempt at intubation is
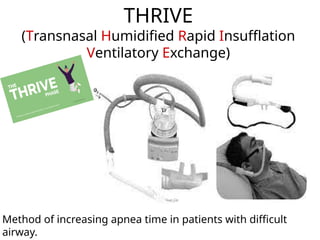
unsuccessful. Transnasal humidified rapid insufflations of oxygen at 70 L/min (transnasal
humidified rapid insufflation ventilatory exchange) should be used when available. No
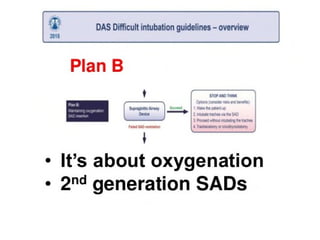
more than three attempts at tracheal intubation and two attempts at supraglottic airway
device (SAD) insertion if intubation fails, provided oxygen saturation remains 95%.
≥
Intubation should be confirmed by capnography. Blind tracheal intubation through the
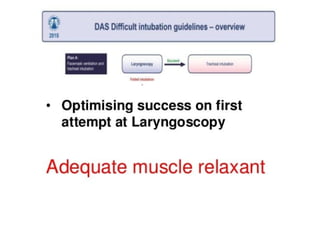
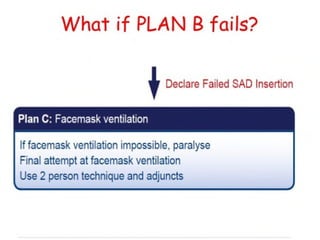
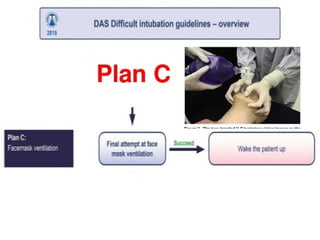
SAD is not recommended. If SAD insertion fails, one final attempt at mask ventilation
should be tried after ensuring neuromuscular blockade using the optimal technique for
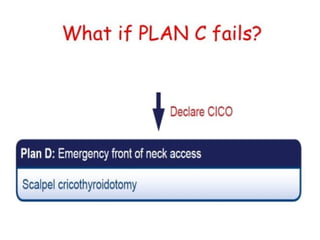
mask ventilation. Failure to intubate the trachea as well as an inability to ventilate the
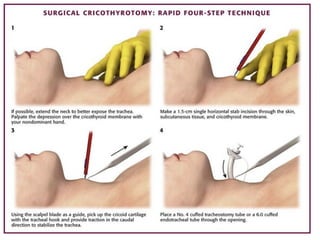
lungs by face mask and SAD constitutes ‘complete ventilation failure’, and emergency
cricothyroidotomy should be performed.
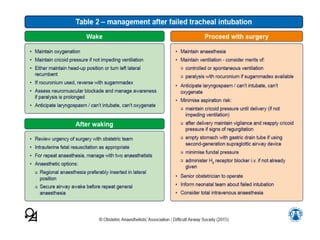
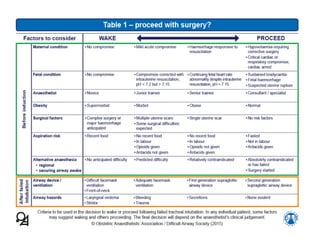
SUMMARY























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







