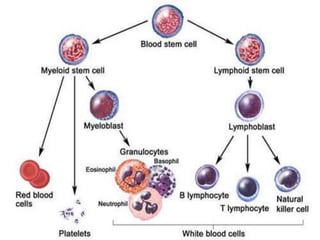
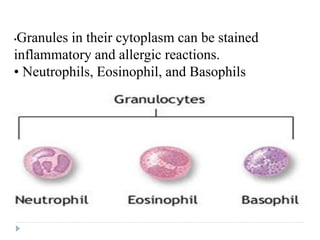
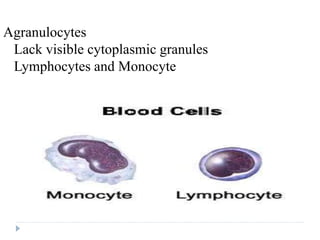
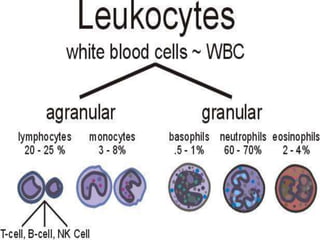
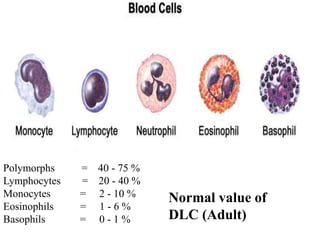
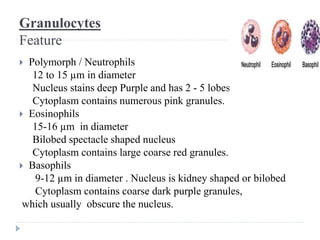
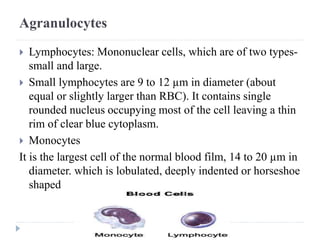
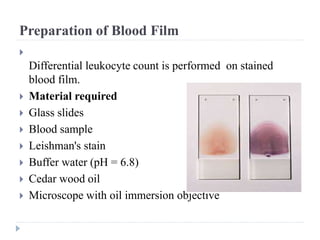
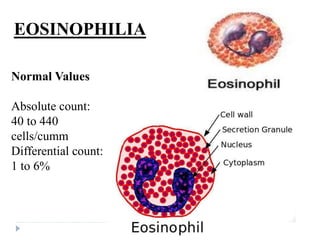
This document discusses a differential leucocyte count (DLC) test. It provides information on the types of white blood cells (WBCs), how a blood smear is prepared and stained, and how the different WBCs are identified and counted under a microscope. A DLC involves counting 100 WBCs and recording the percentages of neutrophils, lymphocytes, monocytes, eosinophils, and basophils present. Normal ranges for each cell type are provided. Eosinophilia, an elevated eosinophil count, and its physiological and pathological causes are also summarized.