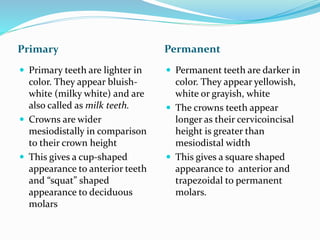
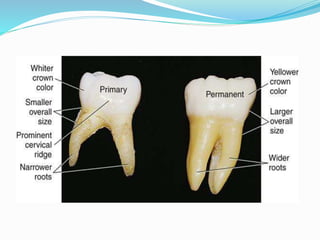
The document presents a comprehensive overview of the differences between primary (deciduous) and permanent dentition, highlighting aspects such as eruption times, crown morphology, clinical significance, and anatomical variations. It discusses the characteristics of teeth, including enamel and dentin properties, pulp anatomy, and root structures, emphasizing their significance in dental procedures. Additionally, the conclusion underscores the importance of understanding these differences for effective dental treatment.
















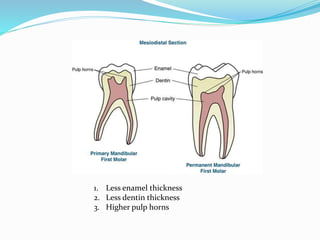





































![Anatomical landmarks of maxilla and mandible [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/anatomicallandmarksofmaxillaandmandibleautosaved-200820132830-thumbnail.jpg?width=640&height=640&fit=bounds)