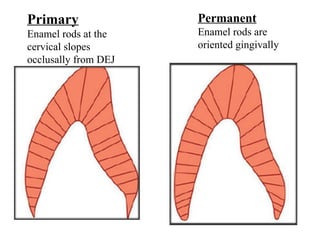
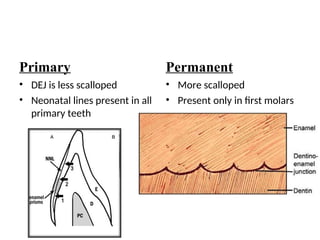
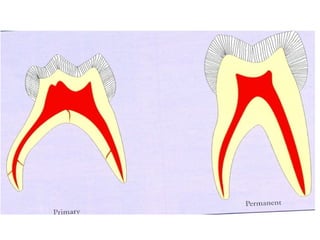
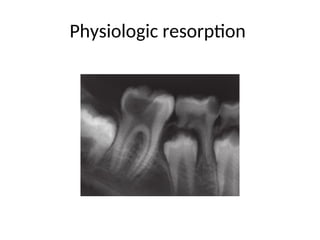
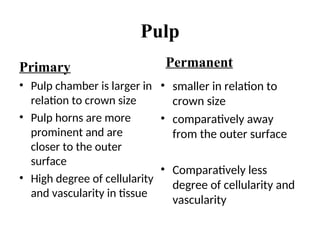
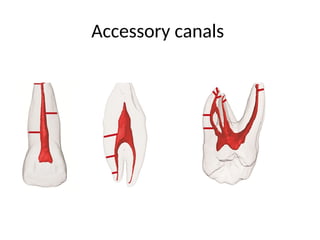
The document compares primary and permanent teeth regarding their characteristics such as color, size, enamel, dentin, pulp, and periodontium. Primary teeth are smaller, lighter, and less mineralized, while permanent teeth are larger, darker, and more mineralized. Key distinctions include differences in structure and potential for repair, as well as the presence of certain features like mamelons and accessory canals.