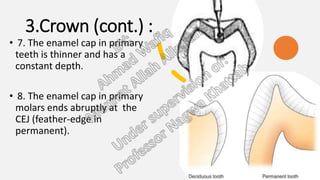
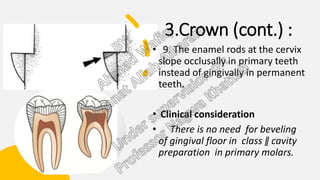
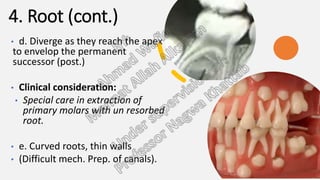
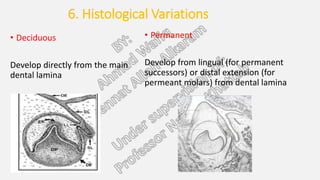
The document summarizes the key morphological differences between deciduous (primary) and permanent teeth. It discusses differences in size, color, crown shape, roots, pulp structure, and histological variations. Primary teeth are smaller, with thinner enamel and dentin. They have shorter, more tapered roots and larger pulp chambers compared to permanent teeth. Histologically, primary teeth develop directly from the dental lamina while permanent teeth develop from extensions, and primary teeth have higher cellularity and innervation than permanent teeth.