Download as PDF, PPTX








![16
medicina
materno
fetal
HNDAC
dialogo: feto-placenta
proteccion o respuestas adaptativas
garantizar el desarrollo fetal en un medio estable
obesity are independent risk factors for neonatal percentage body fat and contribute additively [19
The higher neonatal body fat is of key importance because the number of adipocytes for a huma
being seems to be determined very early in the life cycle if not already in utero [20]. The trajectory
Fig. 1. Proportion (%) of body fat in neonates born to pregnancies with normal glucose tolerance of the mother (NGT) and moth
with gestational diabetes mellitus (GDM). GDM neonates have more body fat not only when born large-for-gestational age (LGA) b
also with appropriate-for-gestational age birth weight (AGA). No data are available for small-for-gestational age (SGA) neonates
GDM pregnancies (left panel). Neonates from lean (BMI < 25) mothers have a lower percentage body fat than their counterpa
born to overweight (BMI 25) mothers (right panel). Data taken from Refs. [15,18].](https://image.slidesharecdn.com/diabetesgestacional-150623220505-lva1-app6892/85/Diabetes-gestacional-16-320.jpg)






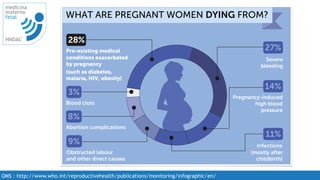
This document discusses gestational diabetes, maternal obesity, and related conditions. It contains the following key points: - Pre-existing medical conditions such as diabetes, obesity, and hypertension exacerbated by pregnancy account for a significant percentage of maternal deaths. - Over the last 30 years, the global prevalence of obesity and diabetes has doubled, with onset of diabetes occurring at younger ages. Gestational diabetes, maternal diabetes, and obesity are associated with adverse outcomes for children. - Early intervention and prevention of gestational weight gain and obesity prior to and during pregnancy can help prevent gestational diabetes and related complications for both mother and baby. Lifestyle intervention programs show promise.

































![Obesity and diabetes [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/obesityanddiabetesautosaved-151216122724-thumbnail.jpg?width=640&height=640&fit=bounds)
![The hapo study[1]](https://cdn.slidesharecdn.com/ss_thumbnails/thehapostudy1-121213181349-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)