Downloaded 31 times

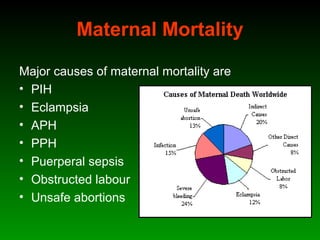








This document discusses identifying and managing high-risk pregnancies. It defines a high-risk pregnancy as one with maternal complications or obstetric risk factors that could threaten the life of the mother or baby. Conducting risk assessments during antenatal care allows early detection of issues and timely referral for specialized care. Key aspects of managing high-risk pregnancies include monitoring for common risks like hypertension and bleeding, providing appropriate medical treatment, and arranging delivery at tertiary care centers that can handle emergencies. A multidisciplinary team approach involving education of mothers is emphasized to provide the best care and reduce mortality risks.



































































