Restriccion del crecimiento Fetal: Manejo basado en estadios
•
15 likes•2,937 views

Exposicion del Dr. Avalos realizada el dia 30 julio 2015

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Restriccion del crecimiento Fetal: Manejo basado en estadios
Similar to Restriccion del crecimiento Fetal: Manejo basado en estadios (20)
More from Hospital Nacional Daniel Alcides Carrión-Callao
More from Hospital Nacional Daniel Alcides Carrión-Callao (9)
Recently uploaded
Recently uploaded (20)
Restriccion del crecimiento Fetal: Manejo basado en estadios
- 1. Dr. Jorge Avalos Restricción de crecimiento Fetal •manejo •consecuencias en la programación fetal
- 2. medicina materno fetal HNDAC Lagercrantz 1997 - The Lancet “Better born too soon than too small”
- 3. medicina materno fetal HNDAC Antenatal identification of SGA and outcome ** ** * * Normal group 20th percentile 10th percentile Moderate SGA Severe SGA Extreme SGA 32 16 8 4 2 1 Grade of weight deviation Riskofseriousfetalcomplication(oddsratio±95%Cl) § §§ Power esti We assum among SG significanc pregnancie halved inc with antep RESULT The numb among tho Compared four-fold i serious feta suffered ad were at an death (eith AGA fetus and extrem (95% CI, 4 OR: 4.1; 95% CI, 2.5–6.8
- 4. medicina materno fetal HNDAC Adaptacion fetal a la insuficiencia placentaria rogramación fetal! ales y papel de la “nutrición” fetal! ! Eduard Gratacos! Medicina Maternofetal i Neonatologia de Barcelona! de Déu i Hospital Clínic, Universitat de Barcelona! ww.medicinafetalbarcelona.org
- 5. Gestación de 14 sem www.medicinafetalbarcelona.org/ Normal and abnormal placental implantation medicina materno fetal HNDAC Programación fetal! es y papel de la “nutrición” fetal! !uard Gratacos! Maternofetal i Neonatologia de B ospital Clínic, Universitat d afetalbarcelona.org resistencia placentariaarteria umbilical arteria uterina <30% de función
- 6. Normal and abnormal placental implantation medicina materno fetal HNDAC Programación fetal! es y papel de la “nutrición” fetal! !uard Gratacos! Maternofetal i Neonatologia de B ospital Clínic, Universitat d afetalbarcelona.org resistencia placentariaarteria umbilical <30% de función disminución flujo vena umbilical crecimiento fetal restringido
- 7. Programación fetal! es y papel de la “nutrición” fetal! !uard Gratacos! Maternofetal i Neonatologia de B ospital Clínic, Universitat d afetalbarcelona.org Normal and abnormal placental implantation medicina materno fetal HNDAC resistencia placentaria arteria umbilical disminución flujo vena umbilical crecimiento fetal restringido redistribucion de flujo arteria cerebral media arteria umbilical arteria cerebral media ICP
- 8. Programación fetal! ales y papel de la “nutrición” fetal! ! Eduard Gratacos! na Maternofetal i Neonatologia de Barcelon Hospital Clínic, Universitat de Barce inafetalbarcelona.org Normal and abnormal placental implantation medicina materno fetal HNDAC resistencia placentaria arteria umbilical disminución flujo vena umbilicalremodelacion cardiaca arteria cerebral media sistole diastole
- 9. Programación fetal! ales y papel de la “nutrición” fetal! ! Eduard Gratacos! na Maternofetal i Neonatologia de Barcelon Hospital Clínic, Universitat de Barce inafetalbarcelona.org Normal and abnormal placental implantation medicina materno fetal HNDAC resistencia placentaria arteria umbilical disminución flujo vena umbilicaldisfuncion cardiaca arteria cerebral media sistole diastoleHTA fetal disfuncion diastolica Doppler pre-cordial
- 10. medicina materno fetal HNDAC Manejo enfocado en estadios y severidad rogramación fetal! ales y papel de la “nutrición” fetal! ! Eduard Gratacos! Medicina Maternofetal i Neonatologia de Barcelona! de Déu i Hospital Clínic, Universitat de Barcelona! ww.medicinafetalbarcelona.org
- 11. Secuencia de deterioro fetal Enfermedad placentaria > impedancia Hipoxia Centralización Hipoxia avanzada Acidosis Injuria severa Muerte fetal Marcadores crónicos Marcadores agudos IP AUt >p95 ICP<p5 IP AU>p95 IP ACM<p5 IP IAo >p95 DV >p95 cCTG <3ms PBF <4 CTG dips DV DRv AU DAu AU DRv ción de 14 sem tal ratio is more UA or MCA alone CPR <p5 0 = IVIIIIII cCTG%STV<3*ms Pathological' CGT www.fetalmedicinebarcelona.org/ Fetal I+D Protocol early-onset IUGR Sequence Doppler (and CTG) changes CPR <p5 Ut A >p95 MCA <p5 DV (a rev) CGT decelerations of reduced short-term variability REDVDV >p95 UVpuls r normal but EFW<p3 Increased resistance Initial redistribution increased resistance and/or redistribution modynamic alteration V High risk of death AEDV AoI >p95
- 12. Enfermedad placentaria > impedancia Hipoxia Centralización Hipoxia avanzada Acidosis Injuria severa Muerte fetal Marcadores crónicos Marcadores agudos IP AUt >p95 ICP<p5 IP AU>p95 IP ACM<p5 IP IAo >p95 DV >p95 cCTG <3ms PBF <4 CTG dips DV DRv AU DAu AU DRv ción de 14 sem tal ratio is more UA or MCA alone CPR <p5 0 = IVIIIIII cCTG%STV<3*ms Pathological' CGT www.fetalmedicinebarcelona.org/ Fetal I+D Protocol early-onset IUGR Sequence Doppler (and CTG) changes CPR <p5 Ut A >p95 MCA <p5 DV (a rev) CGT decelerations of reduced short-term variability REDVDV >p95 UVpuls r normal but EFW<p3 Increased resistance Initial redistribution increased resistance and/or redistribution modynamic alteration V High risk of death AEDV AoI >p95
- 13. Enfermedad placentaria > impedancia Hipoxia Centralización Hipoxia avanzada Acidosis Injuria severa Muerte fetal Marcadores crónicos Marcadores agudos IP AUt >p95 ICP<p5 IP AU>p95 IP ACM<p5 IP IAo >p95 DV >p95 cCTG <3ms PBF <4 CTG dips DV DRv AU DAu AU DRv ción de 14 sem tal ratio is more UA or MCA alone CPR <p5 0 = IVIIIIII cCTG%STV<3*ms Pathological' CGT www.fetalmedicinebarcelona.org/ Fetal I+D Protocol early-onset IUGR Sequence Doppler (and CTG) changes CPR <p5 Ut A >p95 MCA <p5 DV (a rev) CGT decelerations of reduced short-term variability REDVDV >p95 UVpuls r normal but EFW<p3 Increased resistance Initial redistribution increased resistance and/or redistribution modynamic alteration V High risk of death AEDV AoI >p95 LEVE ALTOMEDIO RIESGO DE PREMATURIDAD
- 16. ogramación fetal! y papel de la “nutrición” fetal! ! d Gratacos! ernofetal i Neonatologia de Barcelon al Clínic, Universitat de Barce barcelona.org RCIU mortalidad daño neurologico madurez fetal ingreso UCI-NPrematuridad daño por insuficiencia placentaria Edad gestacional
- 17. www.medicinafetalbarcelona.org/ Programación fetal! Evidencias actuales y papel de la “nutrición” fetal! ! Eduard Gratacos! BCNatal – Centre de Medicina Maternofetal i Neonatologia de Barcelona! Hospital Sant Joan de Déu i Hospital Clínic, Universitat de Barcelona! www.medicinafetalbarcelona.org RCIU mortalidad daño neurologico madurez fetal ingreso UCI-NPrematuridad daño por insuficiencia placentaria Edad gestacional
- 18. ramación fetal! papel de la “nutrición” fetal! ! Gratacos! ofetal i Neonatologia de Barcelona! Clínic, Universitat de Barcelona! rcelona.org RCIU *TRUFFLE 2013 Edad gestacional 26ss 28ss 2% por cada dia mortalidad >90% <10%*20 - 40%* Bashat 2007 30%*superviviencia intacta >50%
- 19. Bashat 2007 Fig. 1. Neonatal survival and in- tact survival rates per gestational week. This figure shows the in- crease in survival (black dia- monds) and intact survival rates until discharge (black bars) in growth-restricted neonates with advancing gestational week. Baschat. Neonatal Outcome in Fetal Growth Restriction. Obstet Gynecol 2007. analysis, neither center of origin nor country of origin influenced the relationship between gestational age, birth weight, and Doppler parameters and neonatal morbidity (Nagelkerke r2 ϭ0.05, Pϭ.796), neonatal death (Nagelkerke r2 ϭ0.09, Pϭ.534) and intact sur- vival (Nagelkerke r2 ϭ0.06, Pϭ.206). DISCUSSION Fetal growth restriction is a prominent contributor to perinatal mortality and morbidities extending all the 1–3,17 intera tion t The a identi anatom sonog Fetal tion a with a Using <26 26-28 DVa'(rev) Yes No IUFD P Cochr Bas mortalidad DV : ausente o reverso: buena correlación con academia mortalidad perinatal : 40 -100% Hecher 1995-2003 Schwarze 2005
- 20. cCTG6STV<3'ms BPP variabilidad a corto plazo STV <3ms marcador agudo de muerte fetal Hecher 2001
- 21. ramación fetal! papel de la “nutrición” fetal! ! Gratacos! ofetal i Neonatologia de Barcelona! Clínic, Universitat de Barcelona! rcelona.org RCIU *TRUFFLE 2013 Edad gestacional 26ss 28ss 2% por cada dia mortalidad >90% <10%*20 - 40%* Bashat 2007 30%*superviviencia intacta >50% Solo indicación materna DVa'(rev) CGT cCTG6STV<3'ms Pathological' CGT DV ar STV<3ms
- 22. www.medicinafetalbarcelona.org/ Programación fetal! Evidencias actuales y papel de la “nutrición” fetal! ! Eduard Gratacos! BCNatal – Centre de Medicina Maternofetal i Neonatologia de Barcelona! Hospital Sant Joan de Déu i Hospital Clínic, Universitat de Barcelona! www.medicinafetalbarcelona.org RCIU mortalidad daño neurologico madurez fetal ingreso UCI-NPrematuridad daño por insuficiencia placentaria Edad gestacional
- 23. www.medicinafetalbarcelona.org/ Programación fetal! Evidencias actuales y papel de la “nutrición” fetal! ! Eduard Gratacos! BCNatal – Centre de Medicina Maternofetal i Neonatologia de Barcelona! Hospital Sant Joan de Déu i Hospital Clínic, Universitat de Barcelona! www.medicinafetalbarcelona.org RCIU mortalidad daño neurologico madurez fetal ingreso UCI-NPrematuridad daño por insuficiencia placentaria Edad gestacional
- 24. 0 15 30 45 60 (%) Controls IUGR antegrade AoI IUGR retrograde AoI Controls IUGR DV<5 z-score IUGR DV>5 z-score * * Brain US anomalies in 30w IUGR ramación fetal! papel de la “nutrición” fetal! ! Gratacos! ofetal i Neonatologia de Barcelona! Clínic, Universitat de Barcelona! rcelona.org RCIU Edad gestacional 28ss 32ss >90% <10%*30 - 40%* daño neurologico AUdr después de las 30s los riesgos de obito superan a los de la prematuridad Fouron’2004 Del'Rio'2008 Cruz Martinez'2012
- 25. ramación fetal! papel de la “nutrición” fetal! ! Gratacos! ofetal i Neonatologia de Barcelona! Clínic, Universitat de Barcelona! rcelona.org RCIU Edad gestacional 28ss 32ss >90% <10%*30 - 40% daño neurologico 15 30 45 60 (%) Controls IUGR antegrade AoI IUGR retrograde AoI Controls IUGR DV<5 z-score IUGR DV>5 z-score * * Brain US anomalies in 30w IUGR
- 26. www.medicinafetalbarcelona.org/ Programación fetal! Evidencias actuales y papel de la “nutrición” fetal! ! Eduard Gratacos! BCNatal – Centre de Medicina Maternofetal i Neonatologia de Barcelona! Hospital Sant Joan de Déu i Hospital Clínic, Universitat de Barcelona! www.medicinafetalbarcelona.org RCIU mortalidad daño neurologico madurez fetal ingreso UCI-NPrematuridad daño por insuficiencia placentaria Edad gestacional
- 27. www.medicinafetalbarcelona.org/ Programación fetal! Evidencias actuales y papel de la “nutrición” fetal! ! Eduard Gratacos! BCNatal – Centre de Medicina Maternofetal i Neonatologia de Barcelona! Hospital Sant Joan de Déu i Hospital Clínic, Universitat de Barcelona! www.medicinafetalbarcelona.org RCIU mortalidad daño neurologico madurez fetal ingreso UCI-NPrematuridad daño por insuficiencia placentaria Edad gestacional
- 28. ramación fetal! papel de la “nutrición” fetal! ! Gratacos! ofetal i Neonatologia de Barcelona! Clínic, Universitat de Barcelona! rcelona.org RCIU Sotiriadis - Bashat ACOG junio 2015 Edad gestacional 32ss 34ss corticoterapia madurez fetal el neurodesarrollo mejora con la administración de corticoides Paralisis Cerebral Disfuncion severa
- 29. AU diastole ausente precede el deterioro fetal en 1 semana Ferrazi 2002 Doppler sequence in IUGR Ferrazzi et al. are reported. Continuous variables were tested for normality (Shapiro-Wilks test) and then analyzed with Student’s t-test. Categorical variables were analyzed with Fisher’s exact test. P < 0.05 was considered significant. The duration of inten- sive fetal monitoring from admission in the fetal intensive care unit to delivery was expressed as number of days prior to delivery. In each patient, we calculated the number of days prior to delivery when a persistently abnormal velocimetric measurement (i.e. for two consecutive examinations) was identified for the first time. Longitudinal cumulative onset time curves were calculated for each Doppler measurement to describe the proportion of cases with abnormal Doppler measurements during the observation time. To allow for a statistical analysis, umbilical changes from absent to reverse end-diastolic flow (AEDF to REDF) and ductus venosus changes from abnormal wave- form (DV S/a) to reverse a-wave (DV RF) were considered independently, as two different marks of adaptation of pro- gressive severity. Linear regression analysis was used to approximate this biological phenomenon described by the longitudinal cumulative curves. The α-coefficient and the intercept value were calculated and anova and Student’s t-test were carried out to test the differences between the dif- ferent curves. Univariate logistic regression was used to iden- tify which one of the independent variables (fetal weight, gestational age at birth or Doppler changes) was a significant predictor of the dependent variable (perinatal outcome). Additionally, in a subset of nine cases that entered the study with Doppler abnormalities in the UA and middle cerebral artery (MCA) (‘early’ changes), the average incidence rate of subsequent abnormal Doppler findings in other vessels was 0 10 20 30 40 50 60 70 80 90 100 –16 –14 –12 –10 –8 –6 –4 –2 0 Days prior to delivery AbnormalDopplerfindings(%) 262521191411975 Observed fetuses (n) Figure 1 Cumulative onset time curves of Doppler abnormalities for each fetal vessel examined. Time ‘0’ refers to the date of delivery. ᭺, MCA PI; ᮀ, UA AEDF; ᭝, DV S/a; , UA RF; , PA PV; ᭡, DV RF; , AO PV. Abbreviations are given in Table 1. Table 2 Statistical analysis between α-coefficient/intercept ratios of cumulative curves t d.f. P* MCA — UA AEDF 18 24 < 0.0001 UA AEDF — DV S/a 12 24 < 0.0001 DV S/a — PA 5.3 24 < 0.0001 PA — UA RF 2.2 24 < 0.03 UA RF — DV RF 1.0 24 NS DV RF — AO 0.04 24 NS 30 45 60 (%) Controls IUGR antegrade AoI IUGR retrograde AoI Controls IUGR DV<5 z-score IUGR DV>5 z-score * * Brain US anomalies in 30w IUGR Pathological' CGT precede en 1 semana a la alteracion del DV Cruz-Martinez 2011 Figueras 2009
- 30. ramación fetal! papel de la “nutrición” fetal! ! Gratacos! ofetal i Neonatologia de Barcelona! Clínic, Universitat de Barcelona! rcelona.org RCIU Edad gestacional 32ss 34ss corticoterapia madurez fetal 30 45 60 (%) Controls IUGR antegrade AoI IUGR retrograde AoI Controls IUGR DV<5 z-score IUGR DV>5 z-score * * Brain US anomalies in 30w IUGR
- 31. www.medicinafetalbarcelona.org/ Programación fetal! Evidencias actuales y papel de la “nutrición” fetal! ! Eduard Gratacos! BCNatal – Centre de Medicina Maternofetal i Neonatologia de Barcelona! Hospital Sant Joan de Déu i Hospital Clínic, Universitat de Barcelona! www.medicinafetalbarcelona.org RCIU mortalidad daño neurologico madurez fetal ingreso UCI-NPrematuridad daño por insuficiencia placentaria Edad gestacional
- 32. www.medicinafetalbarcelona.org/ Programación fetal! Evidencias actuales y papel de la “nutrición” fetal! ! Eduard Gratacos! BCNatal – Centre de Medicina Maternofetal i Neonatologia de Barcelona! Hospital Sant Joan de Déu i Hospital Clínic, Universitat de Barcelona! www.medicinafetalbarcelona.org mortalidad daño neurologico madurez fetal ingreso UCI-NPrematuridad daño por insuficiencia placentaria Edad gestacional
- 33. ramación fetal! papel de la “nutrición” fetal! ! Gratacos! ofetal i Neonatologia de Barcelona! Clínic, Universitat de Barcelona! rcelona.org RCIU DIGITAT 2011 Edad gestacional 34ss 37-38ss Ingreso UCI-N ausencia de descompensacion fetal 650 SGA >37 weeks Induction GA at delivery 38w (96% indution) Fetal distress 18% Acidosis 12% NICU admission 3% Expectant management GA at delivery 39.4w (50% induction) Fetal distress 20% Acidosis 13% NICU admission 4% Induction versus expectant monitoring for intrauterine growth restriction at term: randomised equivalence trial (DIGITAT). BMJ 2011
- 34. ramación fetal! papel de la “nutrición” fetal! ! Gratacos! ofetal i Neonatologia de Barcelona! Clínic, Universitat de Barcelona! rcelona.org RCIU (NEURO)DEVELOMENTAL DIGITAT 2011 Edad gestacional 34ss 37-38ss Ingreso UCI-N ausencia de descompensacion fetal 292 24-months SGA >37 weeks Induction GA at delivery 38w Abnormal neurodevelopment* 25% Abnormal neurobehavior 14% Expectant management GA at delivery 39.4w Abnormal neurodevelopment 29% Abnormal neurobehavior 11% Effects on (neuro)developmental and behavioral outcome at 2 years of age of induced labor compared with expectant management in intrauterine growth-restricted infants: long-term outcomes of the DIGITAT trial. AJOG 2012 Severe IUGR Admission Neonatal Unit
- 35. ramación fetal! papel de la “nutrición” fetal! ! Gratacos! ofetal i Neonatologia de Barcelona! Clínic, Universitat de Barcelona! rcelona.org RCIU Edad gestacional 34ss 37-38ss Ingreso UCI-N ausencia de descompensacion fetal Termino electivo Late-onset IUGR c Constitutional SGA * (UtA)1st visit +UA+MCA Late-onset IUGR c Constitutional SGA * (UtA)1st visit +UA+MCA 1st visit Late-onset IUGR c Constitutional SGA * (UtA)1st visit +UA+MCA ** (UtA)1st visit +UA+MCA+DV
- 36. ramación fetal! papel de la “nutrición” fetal! ! Gratacos! ofetal i Neonatologia de Barcelona! Clínic, Universitat de Barcelona! rcelona.org RCIU Edad gestacional 34ss 37ss Manejo basado en estadios www.medicinafetalbarcelona.org/docencia Late-onset IUGR c Late-onsetIUGR:follow-up Dopp Dopp Dopp Dopp Constitutional SGA * (UtA)1stvisit+UA+MCA **(UtA)1stvisit+UA+MCA+DVwww.medicinafetalbarcelona.org/docencia Late-onset IUGR c Late-onsetIUGR: follow-up Dopp Dopp Dopp Dopp Constitutional SGA * (UtA)1st visit +UA+MCA ** (UtA)1st visit +UA+MCA+DV www.medicinafetalbarcelona.org/docencia Late-onset IUGR c Late-onset IUGR: follow-up Dopp Dopp Dopp Dopp Constitutional SGA * (UtA)1st visit +UA+MCA ** (UtA)1st visit +UA+MCA+DV 30ss26ss 28ss (rev) cal' IUFD 23% in BP Poor correl Cochrane: poor cVa'(rev) cCTG6STV<3'ms ogical' T BPP IUFD 23% in BPP=6 and 11% in BPP=8 Poor correlation with DVa(rev) Cochrane: poor contribution to prediction<29 29-32 >32.0 0 15 30 45 60 (%) Controls IUGR antegrade AoI IUGR retrograde AoI Controls IUGR DV<5 z-score IUGR DV>5 z-score * * Brain US anomalies in 30w IUGR 0 15 30 45 60 (%) Controls IUGR antegrade AoI IUGR retrograde AoI Controls IUGR DV< IUGR DV> * Brain US anomalies in 30w marcadores agudos: muerte fetal / daño neurológico diagnostico Alta sospecha acidemia baja sospecha acidemia Insf. placentaria sev. Inf. plac. leve Parto por cesarea induccion diario 1-2 dias 2v semanal semanal IIIIIIIV
- 37. medicina materno fetal HNDAC ogramación fetal! s y papel de la “nutrición” fetal! !rd Gratacos! ternofetal i Neonatologia de Ba pital Clínic, Universitat de talbarcelona.org RCIU: consecuencias en la programación fetal
- 38. medicina materno fetal HNDAC Programación fetal! ctuales y papel de la “nutrición” fetal! ! Eduard Gratacos! Medicina Maternofetal i Neonatologia de e Déu i Hospital Clínic, Universitat medicinafetalbarcelona.or Reorganizacion cerebral Remodelacion cardiovascular
- 39. medicina materno fetal HNDAC Remodelacion cardiovascular1986 Barker (MRC Unit, Southampton, UK):! Coronary heart disease mortality rates
- 40. medicina materno fetal HNDAC Redistribuir FlujoRCIU cambios adaptativos cambios epigeneticos Programacion cardiaca alteracion doppler
- 41. medicina materno fetal HNDAC RCIU postnatal persistance of cardiovascular remodeling fetal cardiac dysfunction cardiovascular disease in adultho INTRAUTERINE GROWTH RESTRICTION hypertension coronary diseas stroke! obesity! diabetes disfuncion cardiaca remodelacion cardiaca persiste infancia Enfermedad cardiaca en el adulto HTA enfermedad coronaria obesidad ACV diabetes
- 42. medicina materno fetal HNDAC RCIU Skilton&Lancet&2007,&Crispi&Circula6on&2010,&Crispi&AJOG&2012 Cardiovascular, remodeling control IUGR TA)90/65 cIMT = 0.386 mm TA)115/80 cIMT = 0.434 mm postnatal cardiovascular remodelling globular)heart!↓longitudinal)mo;on!↓stroke)volume!↑heart)rate!=)cardiac)output hypertension!preCarteriosclerosis IMPACT,OF,LATE, IUGR/SGA near)term)SGA)fetuses) without)signs)of)poor) prognosis)also) presented)CV) remodeling) Skilton&Lancet&2007,&Crispi&Circula6on&2010,&Crispi&AJOG&2012 Cardiovascular, remodeling control IUGR TA)90/65 cIMT = 0.386 mm TA)115/80 cIMT = 0.434 mm postnatal cardiovascular remodelling globular)heart!↓longitudinal)mo;on!↓stroke)volume!↑heart)rate!=)cardiac)output hypertension!preCarteriosclerosis IMPACT,OF,LATE, IUGR/SGA near)term)SGA)fetuses) without)signs)of)poor) prognosis)also) presented)CV) remodeling) control ART ValenzuelaIAlcaraz&Circula6o decreased)systolic)mo;on impaired)relaxa;on 8 7 6 4 3 0 Rightlongitudinalsystolicmotion!Annularpeakvelocity(S’,cm/s)!Displacement(TAPSE,mm) * 5 1 2 right S’ * TAPSE 80 70 60 40 30 0 Diastolicfunction!Leftisolumetricrelaxationtime(IRT,ms)!RightEdelecelerationtime(Edec,ms) * 50 10 20 E dec * IRT Data)are)median+SEM.)*P<0.05)adjusted)by)GA,)birthweight)cen;le)and)preeclampsia) CONTROL ART Remodelacion Cardiovascular Posnatal Control corazon globular hipertrofia menor movimiento menor volumen eyección incremento FC control ART Valenzu decreased)systolic)mo;on impaired)relaxa;on 8 7 6 4 3 0 Rightlongitudinalsystolicmotion!Annularpeakvelocity(S’,cm/s)!Displacement(TAPSE,mm) * 5 1 2 right S’ * TAPSE 80 70 60 40 30 0 Diastolicfunction!Leftisolumetricrelaxationtime(IRT,ms)!RightEdelecelerationtime(Edec,ms) * 50 10 20 E dec * IRT Data)are)median+SEM.)*P<0.05)adjusted)by)GA,)birthweight)cen;le)and)preeclampsia) Cardiovascular, remodeling control IUGR TA)90/65 cIMT = 0.386 mm TA)115/80 cIMT = 0.434 mm postnatal cardiovascular remodelling globular)heart!↓longitudinal)mo;on!↓stroke)volume!↑heart)rate!=)cardiac)output hypertension!preCarteriosclerosis IMPACT,OF,LATE, IUGR/SGA near)term)SGA)fetuses) without)signs)of)poor) prognosis)also) presented)CV) remodeling) Cardiovascular, remodeling control IUGR TA)90/65 cIMT = 0.386 mm TA)115/80 cIMT = 0.434 mm postnatal cardiovascular remodelling globular)heart!↓longitudinal)mo;on!↓stroke)volume!↑heart)rate!=)cardiac)output hypertension!preCarteriosclerosis IMPACT,OF,LATE, IUGR/SGA near)term)SGA)fetuses) without)signs)of)poor) prognosis)also) presented)CV) remodeling) Hipertension pre-ateroesclerosis
- 43. medicina materno fetal HNDAC RCIU postnatal persistance of cardiovascular remodeling fetal cardiac dysfunction cardiovascular disease in adultho INTRAUTERINE GROWTH RESTRICTION hypertension coronary diseas stroke! obesity! diabetes Predecir????? Prediccion Prevencion Personalizada Participatoria 4P medicina
- 44. medicina materno fetal HNDAC RCIU postnatal persistance of cardiovascular remodeling Barker&BMJ&1986,&Barker&BMJ&1995&,&Hecher&Circula6on&1995,&Crispi&AJOG fetal cardiac dysfunction INTRAUTERINE GROWTH RESTRICTIONPredecir????? Score Cardiovascular Cruz-Lemini 2014
- 45. medicina materno fetal HNDAC A fetal cardiovascular score to predict infant hypertension and arterial remodeling in intrauterine growth restriction Cruz-Lemini, Crispi, Gratacos AJOG 2014 among the different parameters, a hypertension and arterial remodeling in ters continued predictive valu diovascular en ratio (OR, 2.2 .001), right sp 95% CI, 1.4e IVRT (OR, 2.2 .001) had the composite scor best perinatal graphic predict combination o regression anal cular score was score), cerebro right sphericity IVRT (z-score the following e 1:907 þ ðTAP þ ðcerebropl þ ðright sphe þ ðIVRT Â The equatio tivity, 77% s predictive value value, 3.9 posi 0.1 negative li those IUGR ca sion and arter operating char son was perfor FIGURE 1 Univariate analysis for the association between perinatal and fetal echocardiographic parameters with hypertension and arterial remodeling in IUGR infants Hypertension and arterial remodeling were defined as mean blood pressure of >95th percentile and aortic intima media of >75th percentile at 6 months of age. Fetal parameters included as z-scores
- 46. medicina materno fetal HNDAC A fetal cardiovascular score to predict infant hypertension and arterial remodeling in intrauterine growth restriction Cruz-Lemini, Crispi, Gratacos AJOG 2014 FIGURE 2 Components of the fetal cardiovascular score for the prediction of hypertension and arterial remodeling Obstetrics Research GURE 2 omponents of the fetal cardiovascular score for the prediction of ypertension and arterial remodeling Obstetrics Researchperformance than perinatal factors and fetoplacental Doppler scans that were used for establishing the severity of the IUGR. Echocardiographic measurements in fetuses were consistent with previous studies that demonstrated significant differences in cardiac function under IUGR.1-3,5,11,12,32,37-40 Likewise, in- creased blood pressure and aIMT pre- viously had been reported in IUGR neonates and children.3,32,38,40-42 The present study expands previous findings. Longitudinal follow-up evaluations dem- onstrated the relationship between pre- natal echocardiography and postnatal cardiovascular findings. As expected, gestational age and birthweight percentile showed no associ- ationwith the occurrence of hypertension IVRT, isovolumic relaxation time; TAPSE, tricuspid annular-plane systolic excursion. Cruz-Lemini. Fetal echocardiography to predict postnatal hypertension in IUGR. Am J Obs an perinatal factors and oppler scans that were hing the severity of the aphic measurements in onsistent with previous emonstrated significant cardiac function under 2,37-40 Likewise, in- ressure and aIMT pre- en reported in IUGR children.3,32,38,40-42 The pands previous findings. ow-up evaluations dem- lationship between pre- ography and postnatal ndings. gestational age and entile showed no associ- IVRT, isovolumic relaxation time; TAPSE, tricuspid annular-plane systolic excursion. Cruz-Lemini. Fetal echocardiography to predict postnatal hypertension in IUGR. Am J Obstet Gynecol 2014. indice esfericidad ICP TAPSE TRI
- 47. medicina materno fetal HNDAC A fetal cardiovascular score to predict infant hypertension and arterial remodeling in intrauterine growth restriction Cruz-Lemini, Crispi, Gratacos AJOG 2014 trial in a l that the in with arter can be pre suppleme life.49 Among the longi and func ings from allowed u effects of controllin much as p by includ IUGR, ex because o all the s suspected FIGURE 3 Receiver operating characteristic curves illustrating the predictive value of fetal CV score
- 48. medicina materno fetal HNDAC RCIU postnatal persistance of cardiovascular remodeling fetal cardiac dysfunction cardiovascul disease in adult INTRAUTERINE GROWTH RESTRICTION hypertensio coronary dise stroke! obesity! diabetes S:90 - E: 85% Score Cardiovascular Remodelamiento vascular Intervención Estilo de vida Dieta: omega 3 ejercicio hipotensores Williams 2009 Kavey 2006 Skilton 2012-2013
- 49. medicina materno fetal HNDAC Programación fetal! ctuales y papel de la “nutrición” fetal! ! Eduard Gratacos! Medicina Maternofetal i Neonatologia de e Déu i Hospital Clínic, Universitat medicinafetalbarcelona.or Reorganizacion cerebral Remodelacion cardiovascular
- 50. medicina materno fetal HNDAC www.medicinafetalbarcelona.org/ Programación fetal! ncias actuales y papel de la “nutrición” fetal! ! Eduard Gratacos! Centre de Medicina Maternofetal i Neonatologia de Barcelona! ant Joan de Déu i Hospital Clínic, Universitat de Barcelona! www.medicinafetalbarcelona.org Reorganizacion cerebral exposure Fetal&programming& Brain&reorganiza0on& exposure Injuria
- 51. medicina materno fetal HNDAC www.medicinafetalbarcelona.org/ Programación fetal! ncias actuales y papel de la “nutrición” fetal! ! Eduard Gratacos! Centre de Medicina Maternofetal i Neonatologia de Barcelona! ant Joan de Déu i Hospital Clínic, Universitat de Barcelona! www.medicinafetalbarcelona.org Reorganizacion cerebral Normal acoustic signature re Ultrasound texture analysis Normal acoustic signature re Ultrasound texture analysis Cual es normal?
- 52. medicina materno fetal HNDAC Programación fetal! videncias actuales y papel de la “nut ! Eduard Gratac Natal – Centre de Medicina Maternof spital Sant Joan de Déu i Hosp www.med NEW THERAPIES NEW IMAGING IMPROVING NEURODEVELOPMENTAL DISORDERS OF FETAL ORIGIN NOVEL RESEARCH LINES IMPROVING DETECTION NEW THERAPIES DISORDERS OF FETAL ORIGIN NOVEL RESEARCH LINES MPROVING DETECTION NEW THERAPIES NEW IMAGING BIOMARKERS NOVEL RESEARCH LINES MPROVING DETECTION Mejorar Diagnostico Nuevos Biomarcadores nuevas terapias Mejorando el estudio de los origenes fetales del neurodesarrollo
- 53. medicina materno fetal HNDAC Programación fetal! videncias actuales y papel de la “nu ! Eduard Grata Natal – Centre de Medicina Materno spital Sant Joan de Déu i Hos www.me Microestructura CONECTIVIDAD Desarrollo cortical Efectos de la desnutrición Fetal en el neurodesarrollo MICROSTRUCTURE METABOLISM CONNECTIVITY CORTICAL DEVELOPMENT MICROSTRUCTURE METABOLISM CORTICAL DEVELOPMENT MICROSTRUCTURE METABOLISM CONNECTIVITY CORTICAL DEVELOPMENT
- 54. medicina materno fetal HNDAC Microestructura Analisis de Textura MICROSTRUCTURE METABOLISM CONNECTIVITY CORTICAL DEVELOPMENT TEXTURE ANALYSIS Sanz et al. Fet Diagn Ther 2013. FETAL MRI SGAs vs AGA LATE IUGR TEXTURE ANALYSIS Sanz et al. Fet Diagn Ther 2013. FETAL MRI Texture analysis showed brain differences in SGA fetuses that increase VD SGAsSGAs vs AGA LATE IUGR J Ultrasound Med 2011 Fetal Diagn Ther 2012 Am J Obstet Gynecol 2012
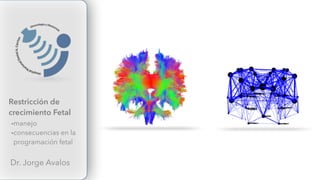
- 55. Medicina Fetal Barcelona 2015 medicina materno fetal HNDAC Programación fetal! videncias actuales y papel de la “n ! Eduard Grat Natal – Centre de Medicina Mater spital Sant Joan de Déu i H www.m Infantes con RCIU muestran disminucion de la conectividad normal RCIU
- 56. Medicina Fetal Barcelona 2012 medicina materno fetal HNDAC Fetus Young OldChild Mature IMPACT OF ENVIRONMENT BIOLOGIC-PROGRAMMING-AND-AGE OPPORTUNITY FOR CORRECTION