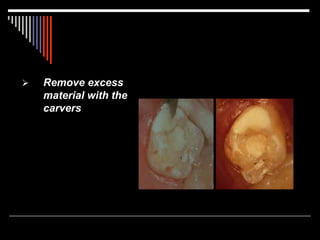
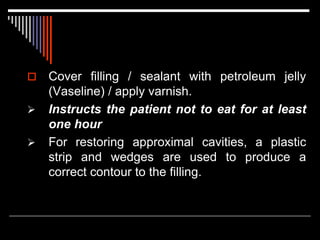
ART (Atraumatic Restorative Treatment) is a minimally invasive dental technique developed in the 1980s as an alternative to traditional drills and fillings. It uses hand instruments to remove decay and restores teeth with adhesive glass ionomer materials. ART was developed for areas without access to traditional dental equipment and materials. It has advantages of being inexpensive, painless, and conserving tooth structure. ART is effective for small cavities but has limitations such as longevity of restorations and acceptance by dental professionals. It provides an alternative for underserved populations worldwide.