Downloaded 44 times

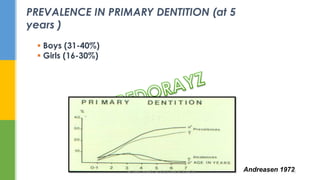


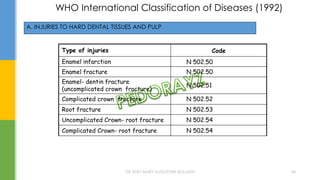
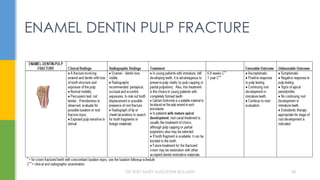
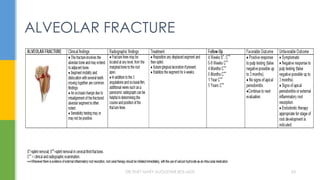
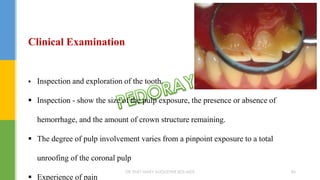
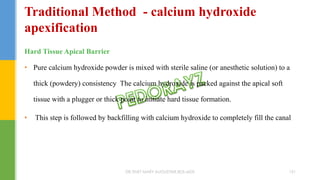
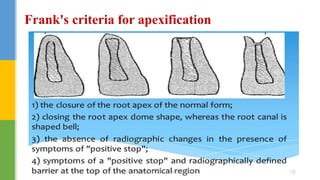
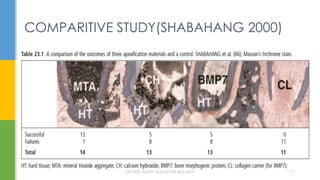
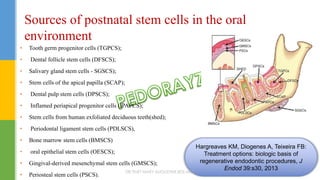
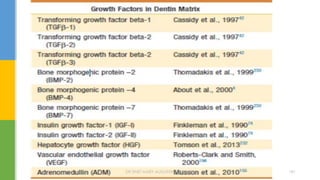
![Modified Ellis classification
[By McDonald, Avery and Lynch(1983)]
Class I - Simple fracture of crown , involving little or no dentin
Class II - Extensive fracture of the crown involving considerable dentin but
not the dental pulp
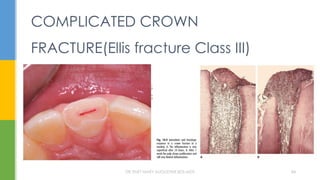
Class III - - Extensive fracture of the crown involving considerable dentin and
exposing the pulp
Class IV - loss of the entire crown
DR.TINET MARY AUGUSTINE.BDS.MDS 37](https://image.slidesharecdn.com/crownfracture-191120094221/85/Dental-Crown-fracture-37-320.jpg)



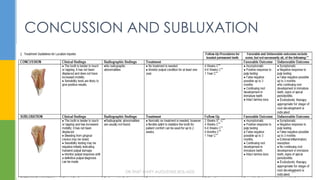





![• Zinc oxide-eugenol cements
• Polycarboxylate cements
• Collagen
• Calcium hydroxide (Ca[OH]2
• Bonding agents
• Glass Ionomer Cements
• Mineral Trioxide Aggregate (MTA)
• Biodentine
• Emdogain
• Propolis
• Endosequence.
MEDICAMENTS
DR.TINET MARY AUGUSTINE.BDS.MDS 104](https://image.slidesharecdn.com/crownfracture-191120094221/85/Dental-Crown-fracture-104-320.jpg)

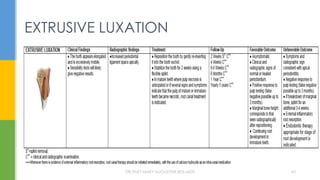
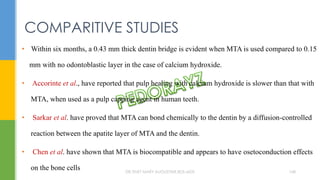
![MTA reveals very good sealing properties in dry and blood
contaminated environments [Maturo et al., 2009].
MTA
DR.TINET MARY AUGUSTINE.BDS.MDS 110](https://image.slidesharecdn.com/crownfracture-191120094221/85/Dental-Crown-fracture-110-320.jpg)

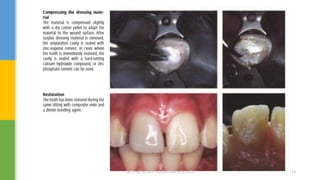


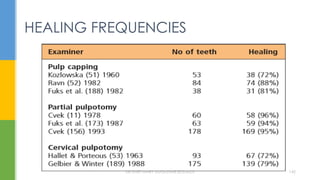
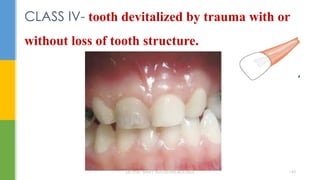






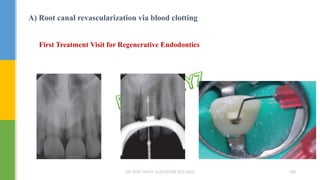





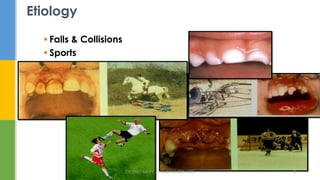
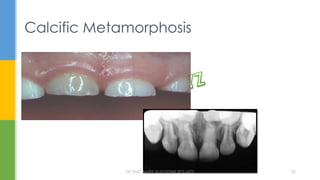
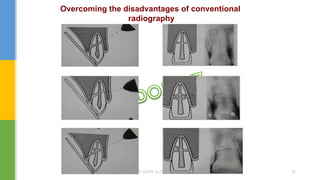
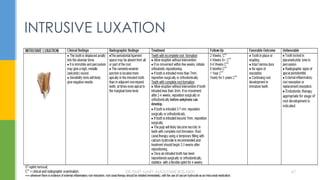
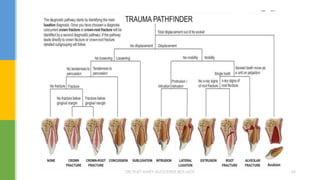
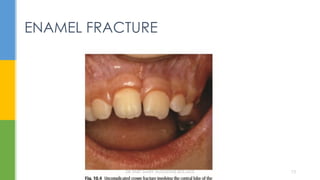
The document discusses traumatic injuries to the permanent dentition, specifically crown fractures. It provides an overview of the etiology, incidence, classification, and management of dental injuries. Key points include that the incidence of dental trauma from accidents and sports has increased in recent decades, commonly affecting the front teeth of children and teenagers. Proper initial treatment is important to promote healing. Classification systems help describe the specific injury and guide clinical decision making.






















































































