Download as PDF, PPTX


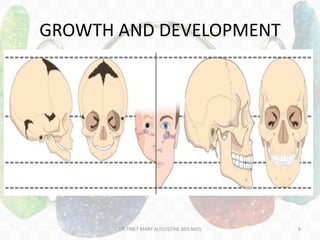

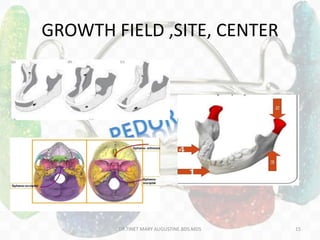
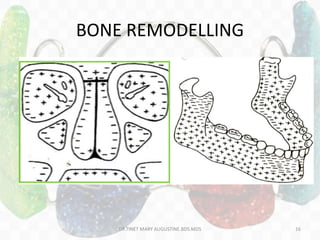
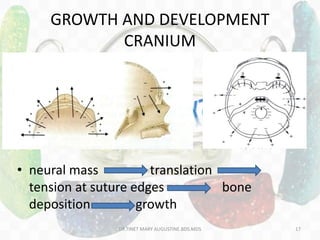
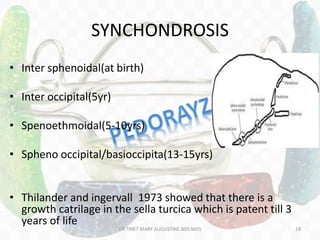








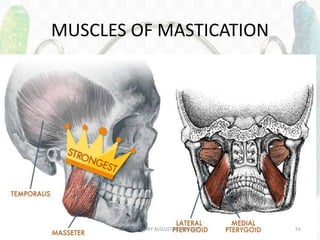
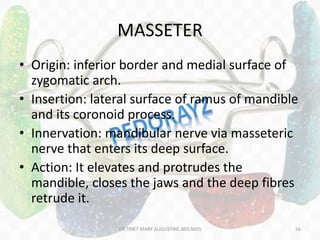
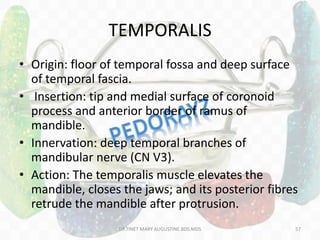
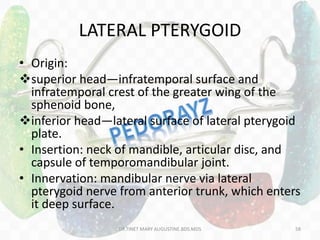
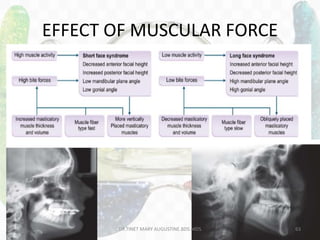
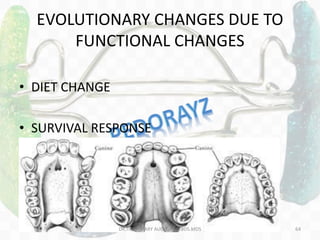
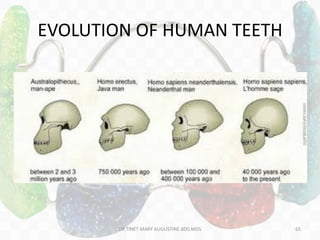
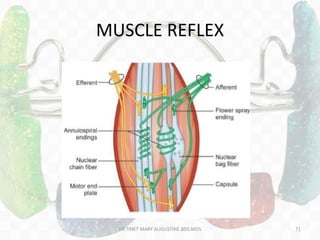
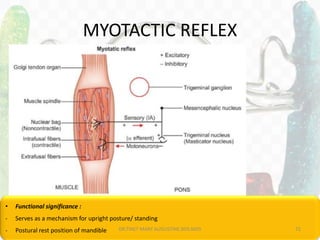
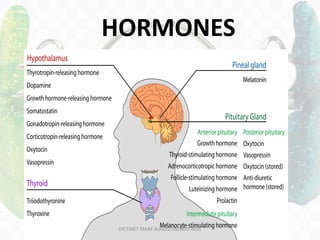
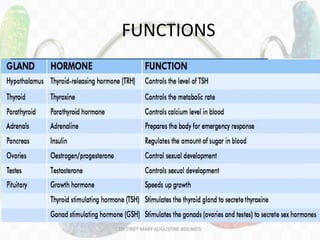
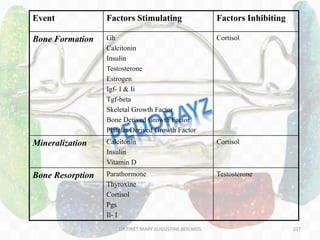






This document discusses myofunctional appliances and the basic principles of myofunctional therapy. It covers topics like normal growth and development of bones, TMJ, muscles and hormones. It describes principles of functional appliances and their role in correcting malocclusion. Different types of functional appliances are listed along with bonding procedures in orthodontics. The document also discusses theories of growth, development of cranial and facial bones, muscles of mastication, TMJ and the effect of muscular force.





















































































