Downloaded 3,340 times
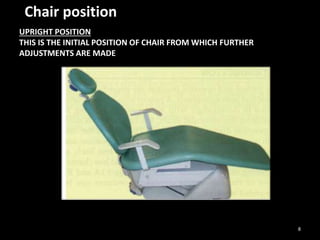
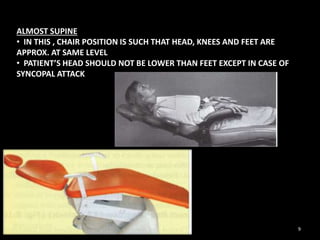
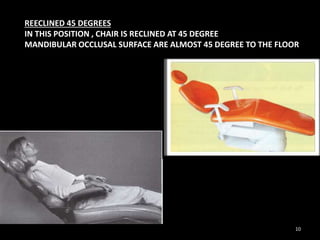
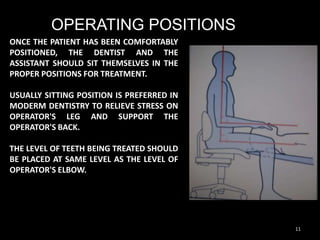
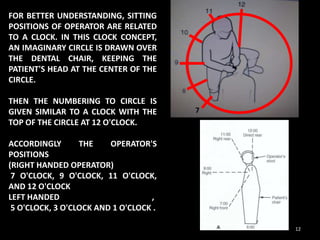
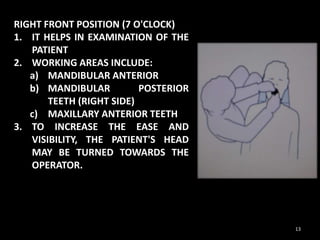
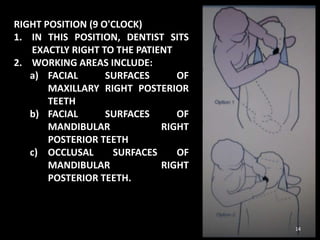
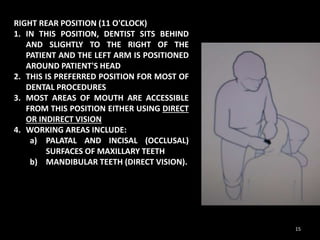
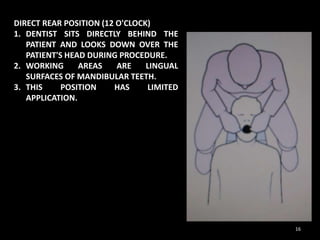
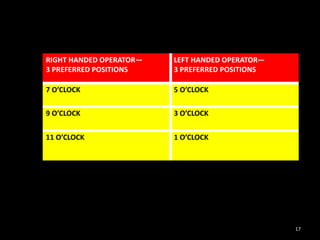
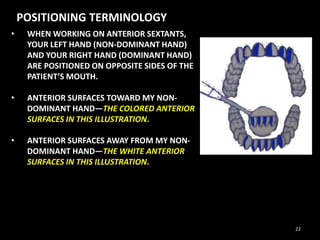
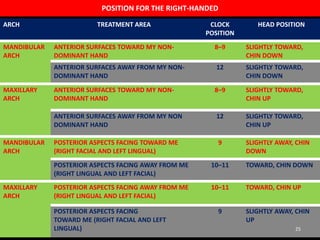
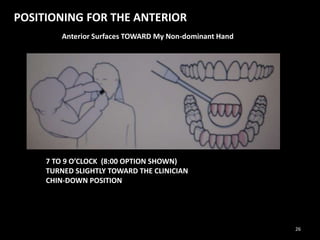
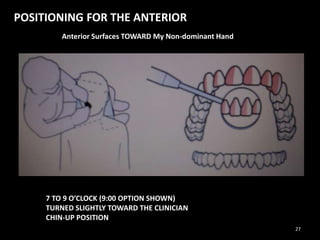
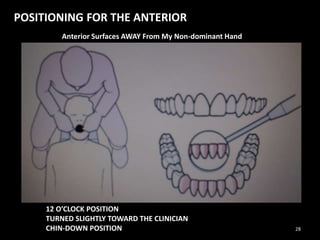
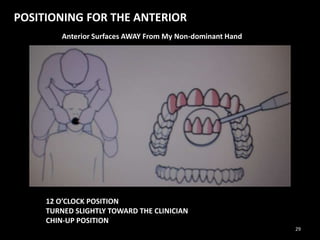
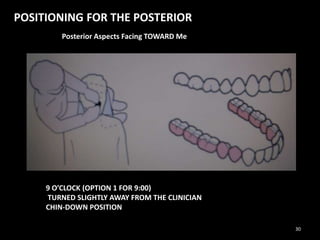
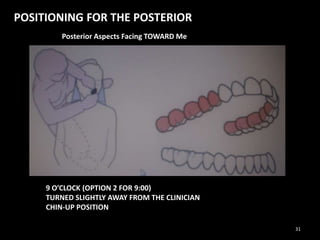
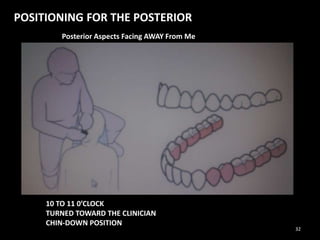
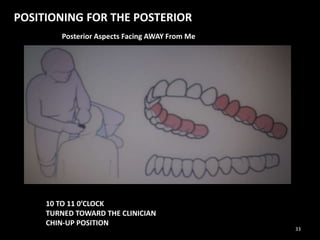


The document discusses dental chair and patient positioning. It describes upright, almost supine, and reclined 45 degree positions for patients. Operating positions for the dentist are defined relative to a clock, including right front (7 o'clock), right (9 o'clock), right rear (11 o'clock), and direct rear (12 o'clock). The sequence for establishing proper positioning is outlined as: 1) operator position, 2) patient chair and head position, 3) equipment adjustment, 4) non-dominant hand placement, and 5) dominant hand placement. Correct positioning is important for operator ergonomics and visibility during dental procedures.











































![Principles of periodontal instrumentation [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/principlesofperiodontalinstrumentationautosaved-210220074109-thumbnail.jpg?width=640&height=640&fit=bounds)




































