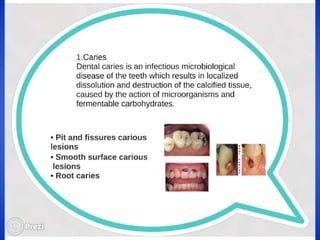
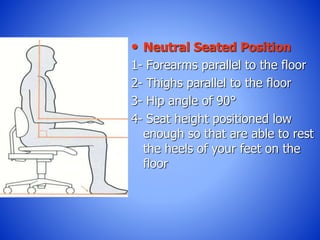
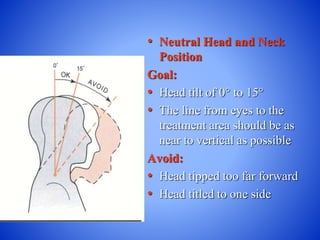
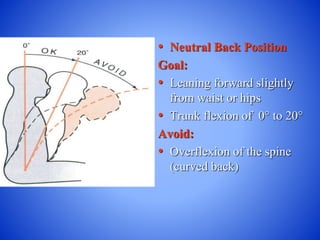
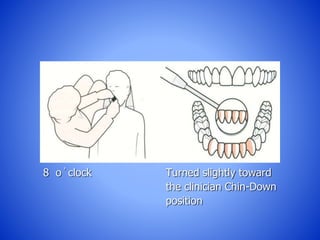
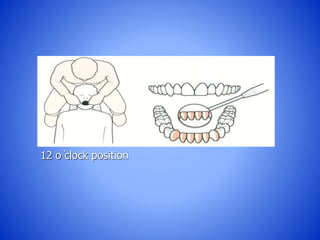
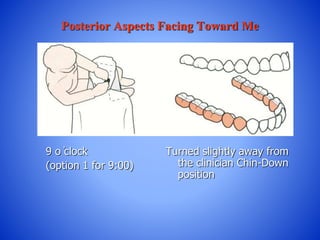
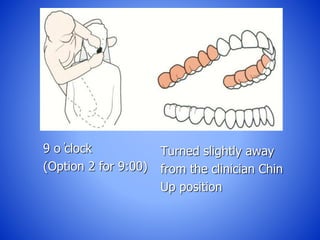
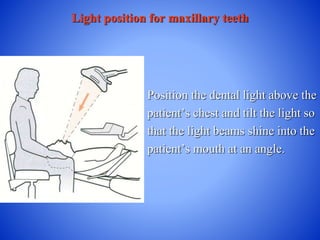
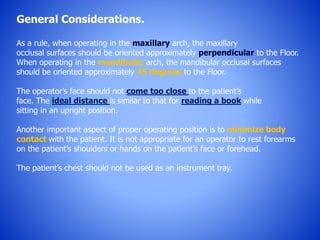
The document outlines the principles and practices of conservative dentistry, focusing on diagnosis, treatment, and management of tooth defects without full coverage restorations. Key objectives include prevention, interception, and restoration while maintaining infection control and optimal patient positioning for effective treatment. It also details operator positioning and light placement strategies to ensure ergonomic and effective dental procedures.