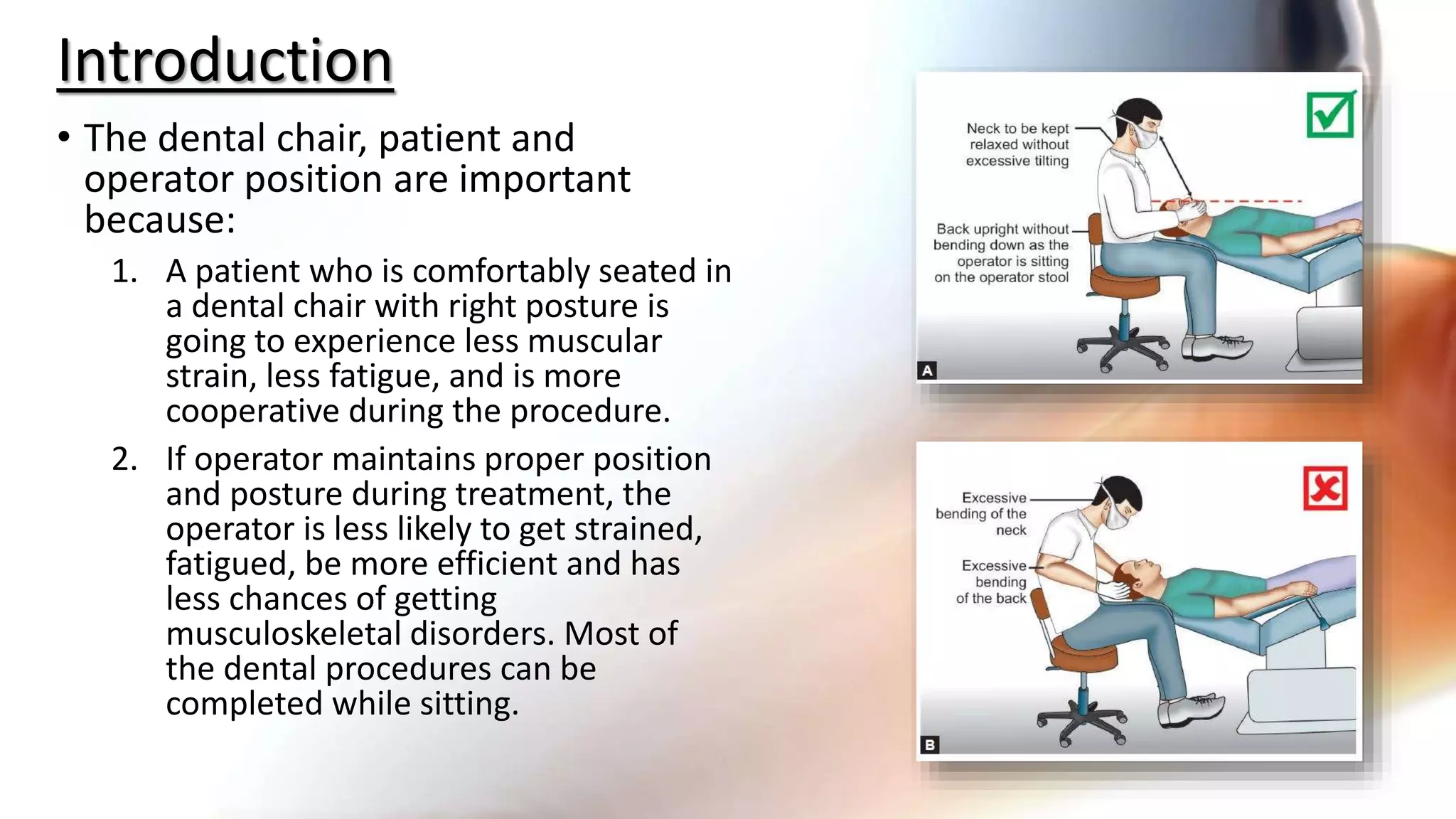
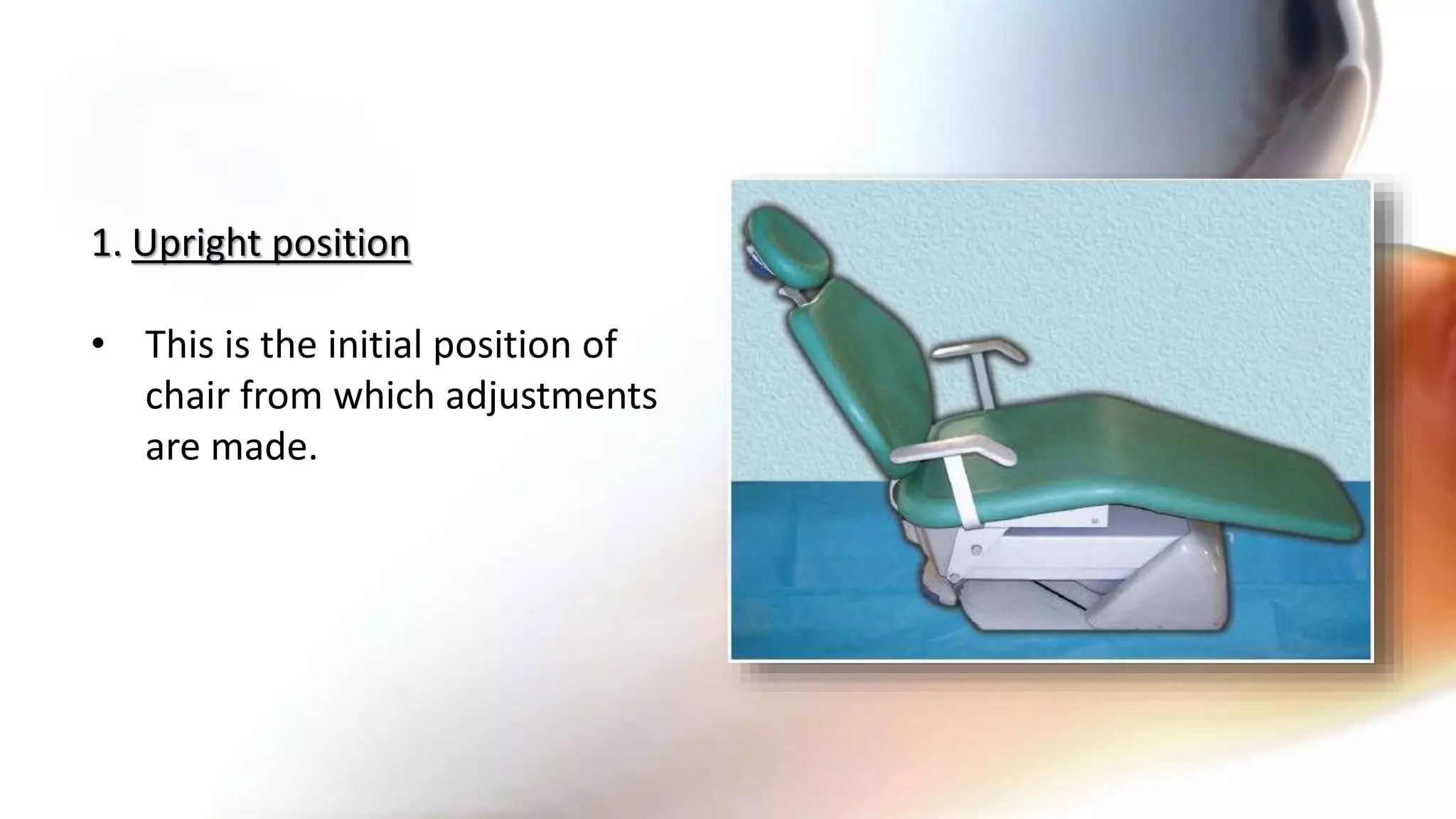
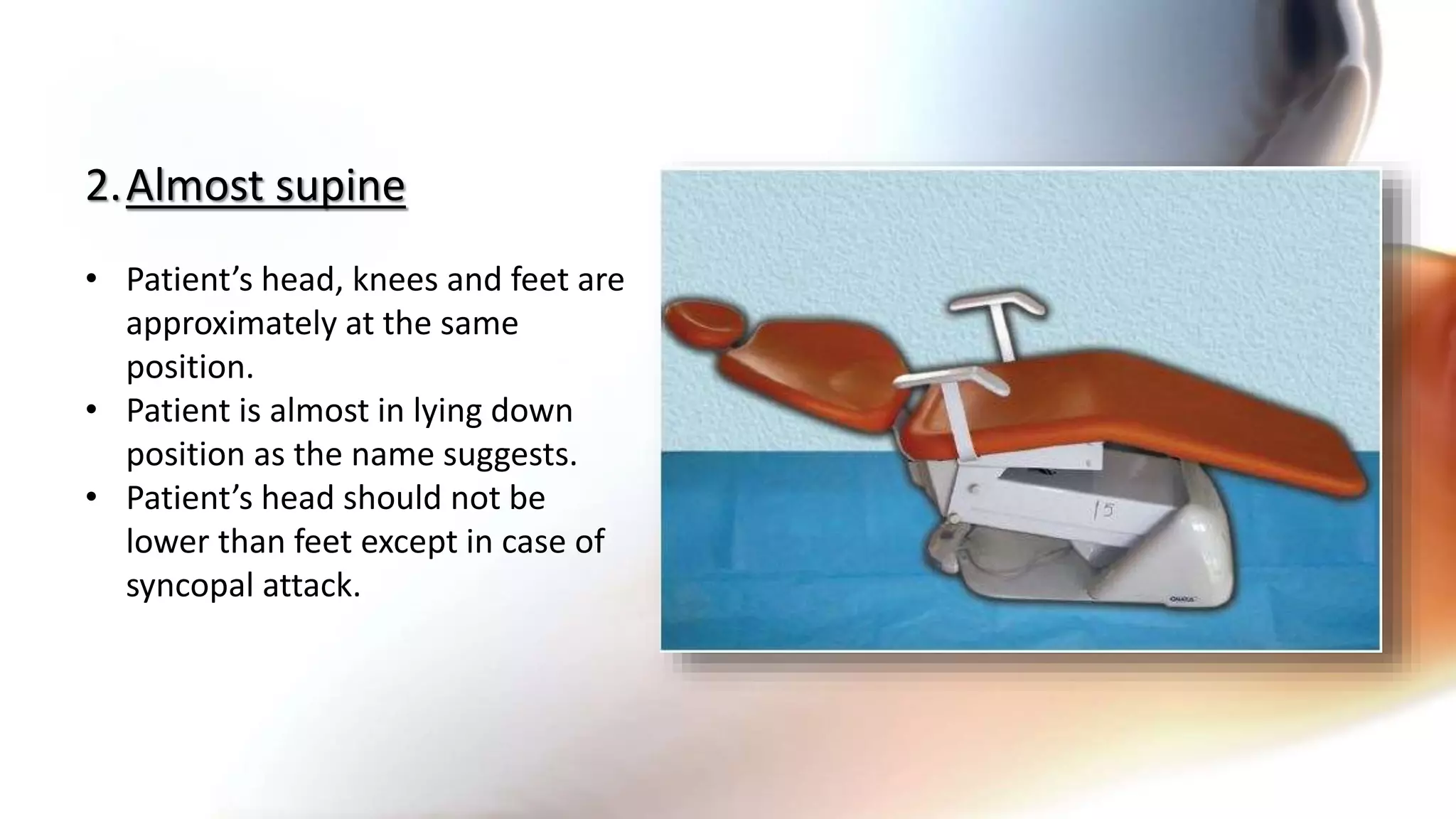
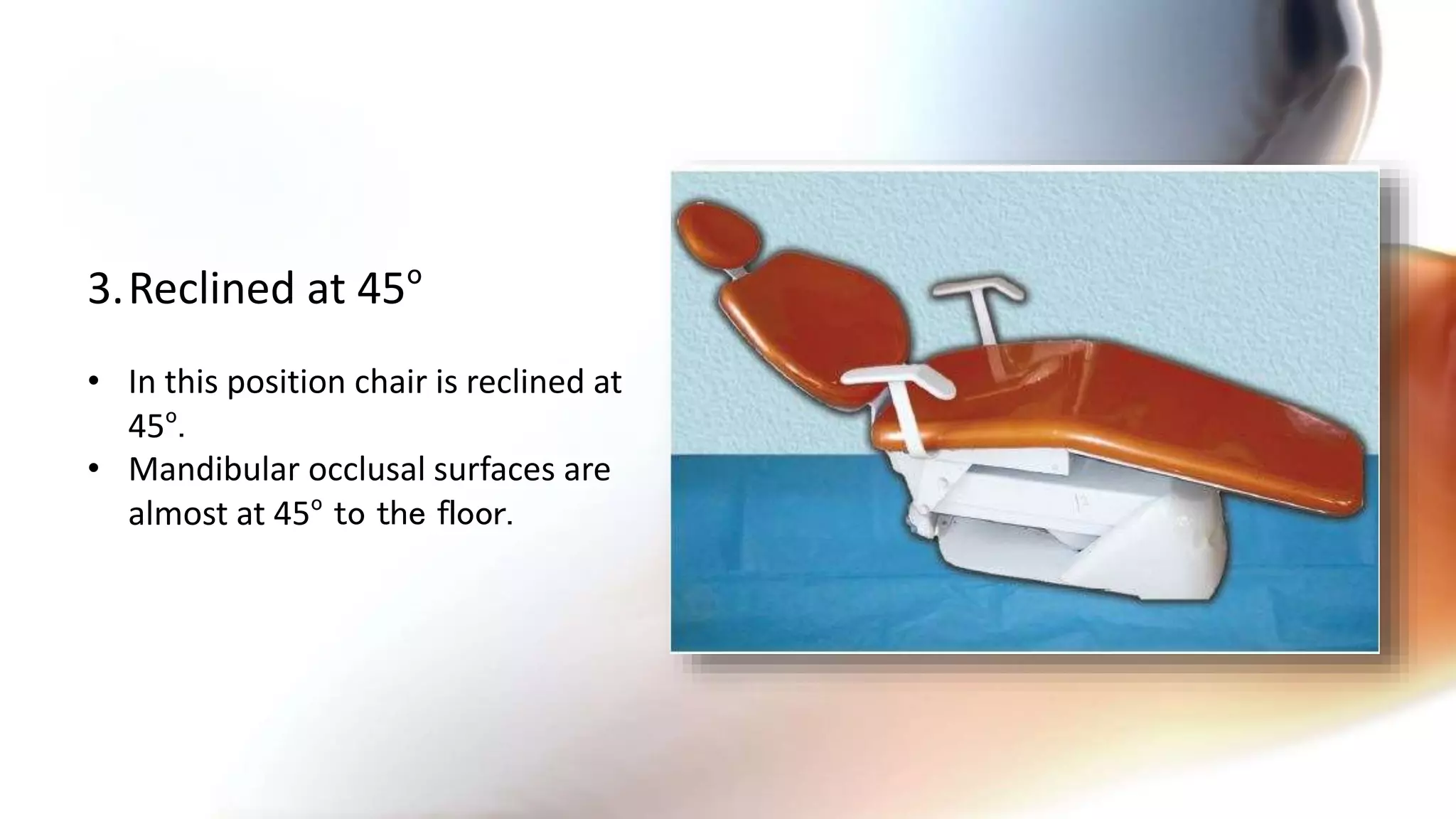
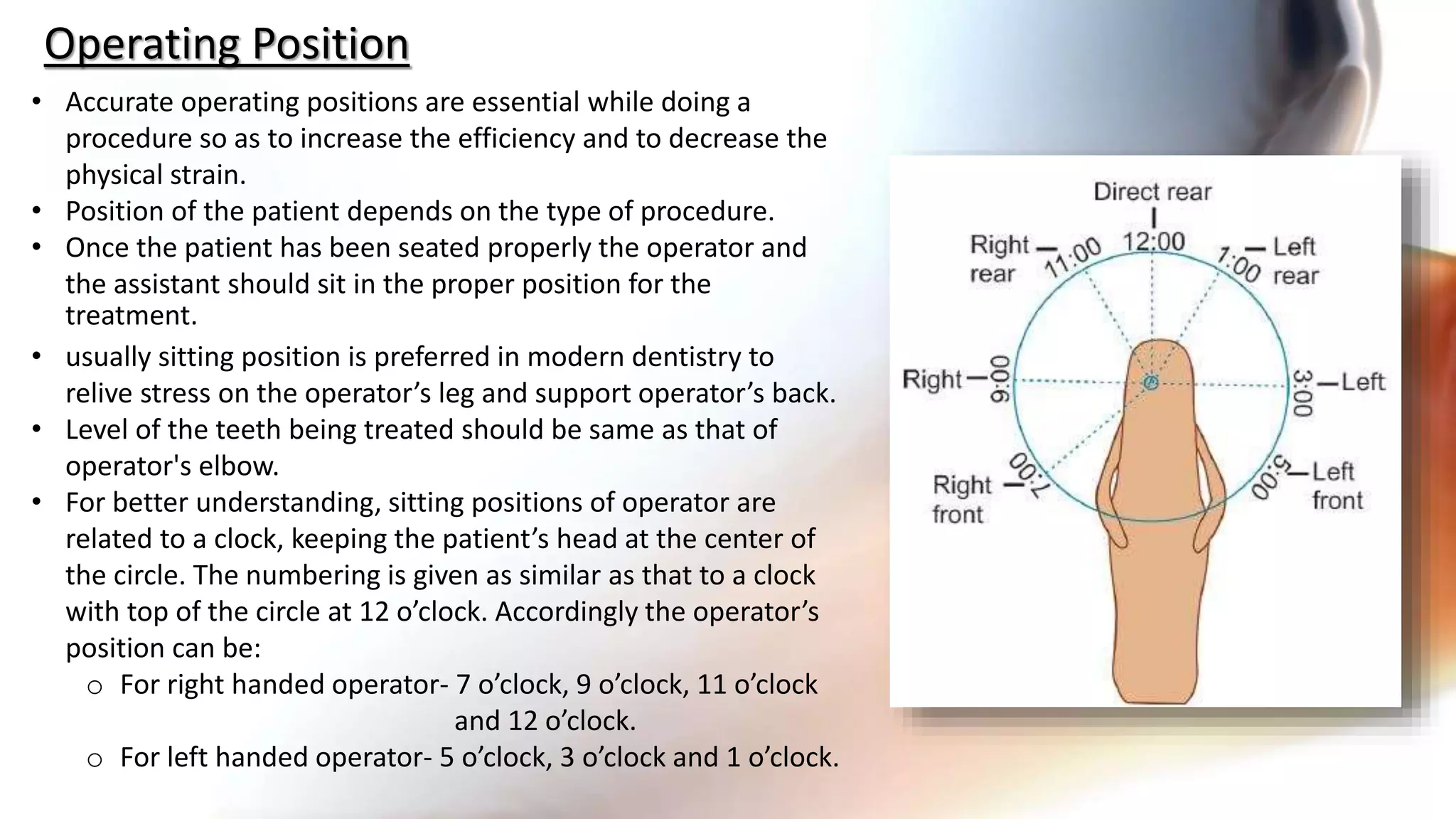
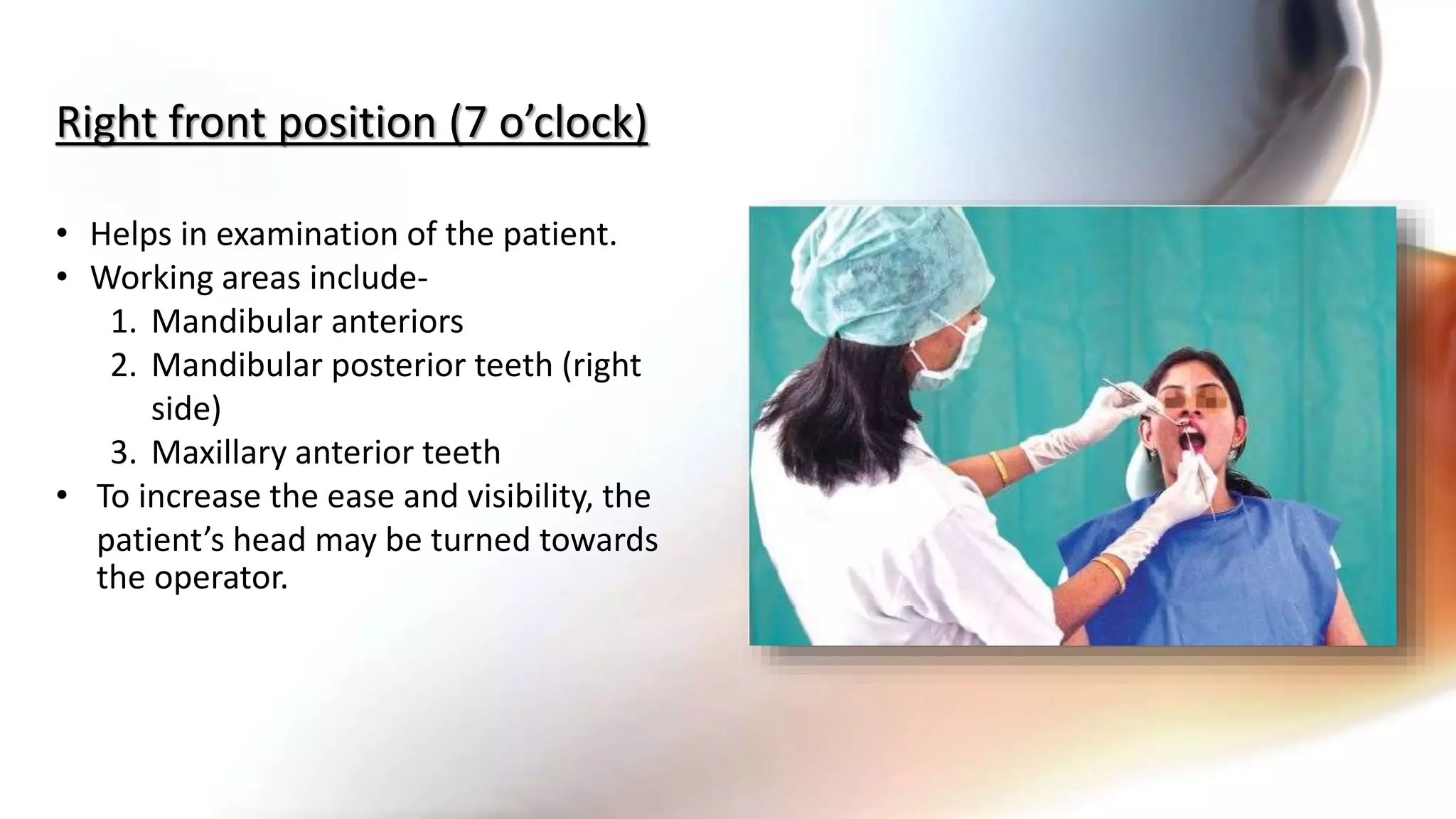
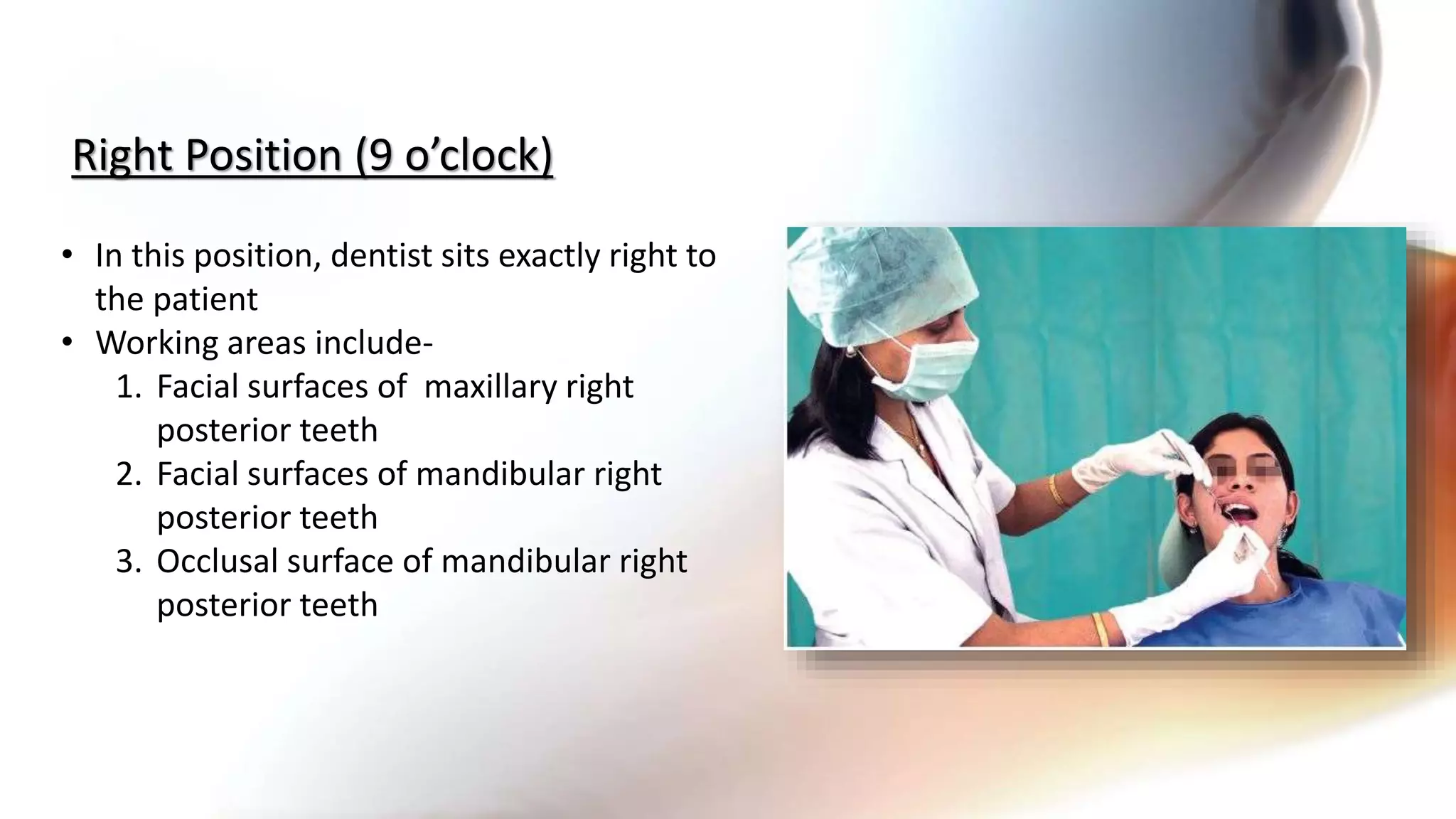
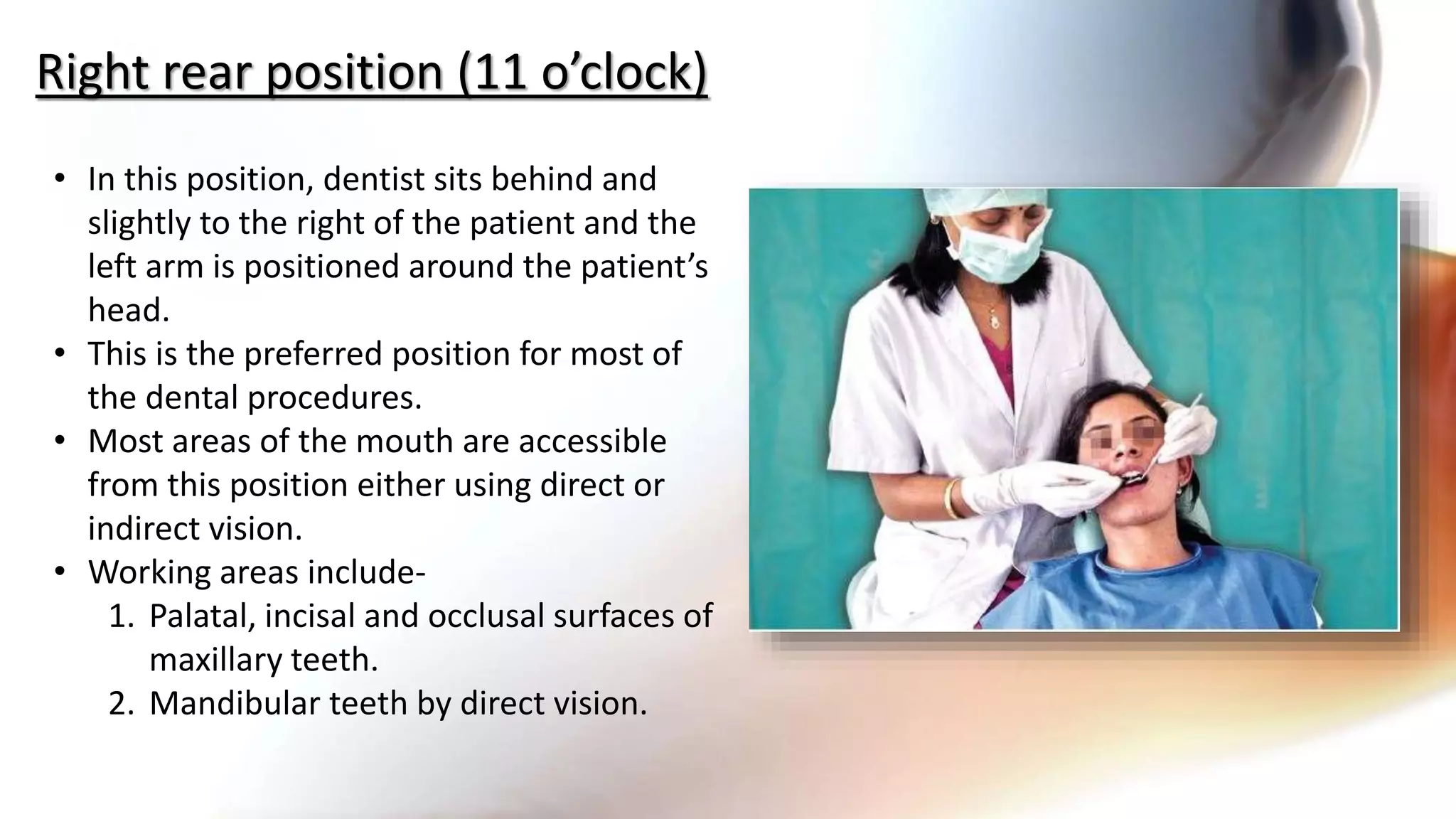
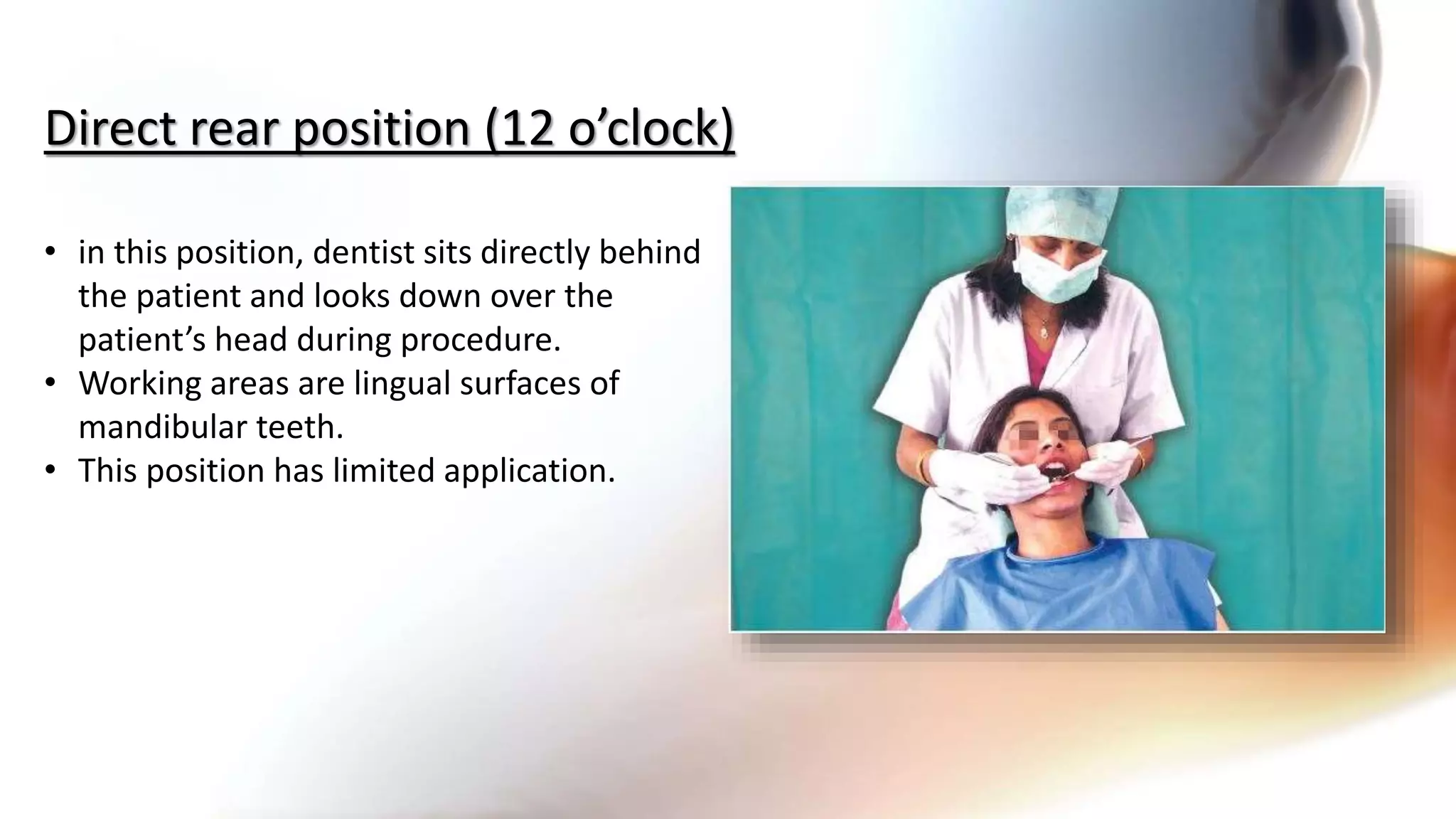
The document discusses the importance of dental chair design and operator positioning for patient comfort and procedural efficiency. It describes various seating positions for patients and dentists, emphasizing ergonomics to minimize strain and increase efficiency during treatments. It also highlights zones of the working area and best practices for instrument exchange and magnification tools to enhance visibility and reduce physical stress during dental procedures.