Downloaded 188 times

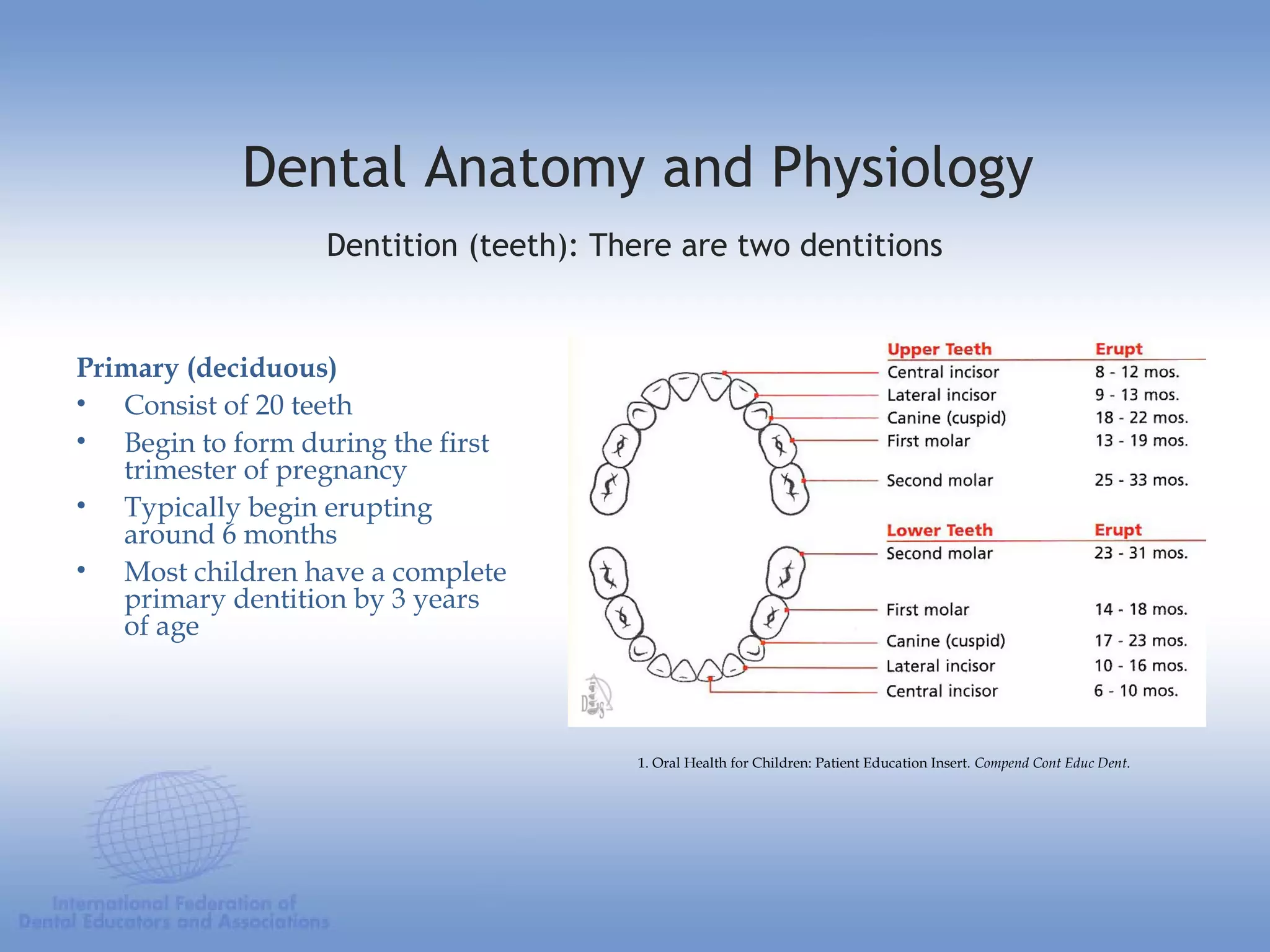

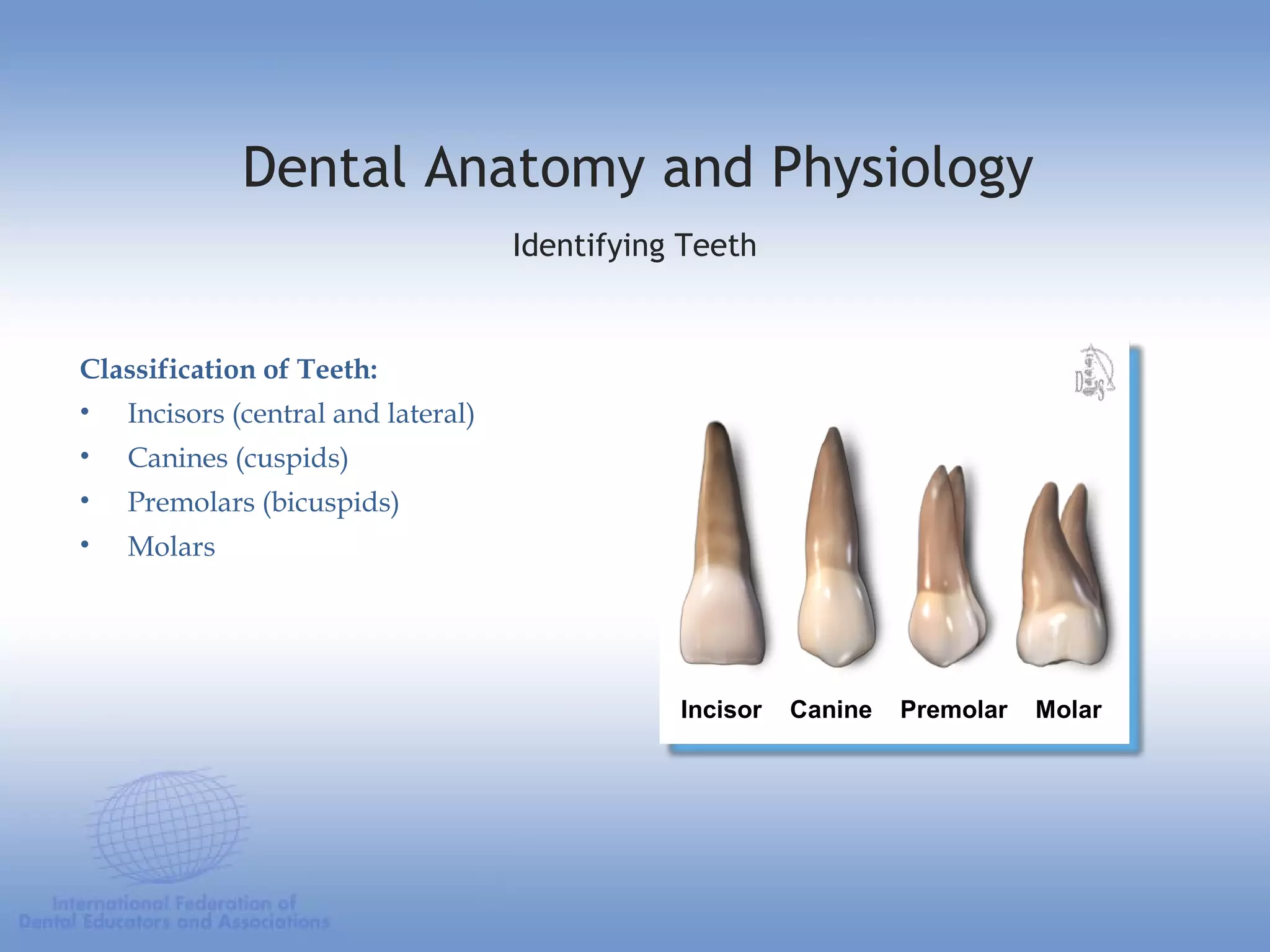


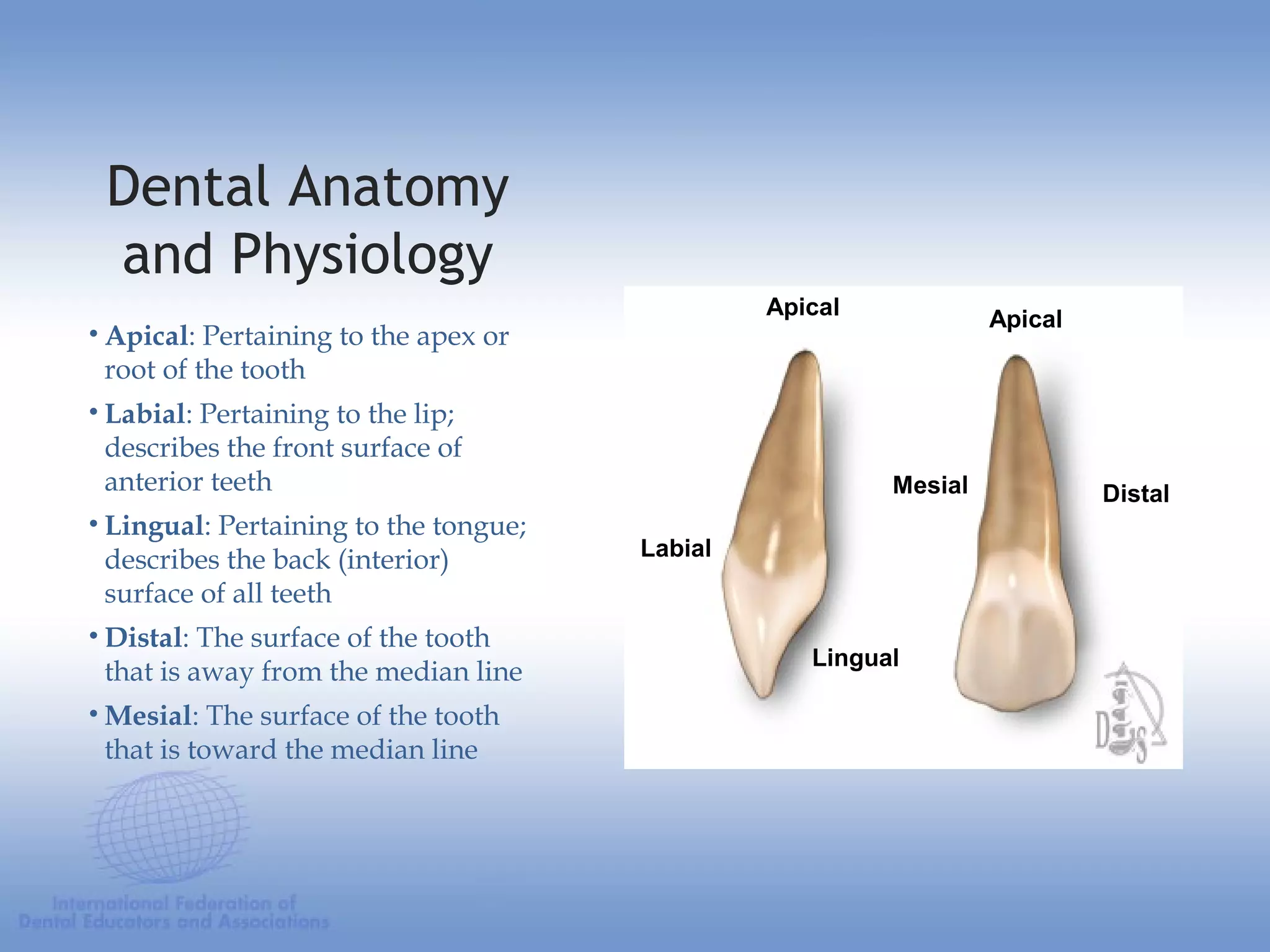
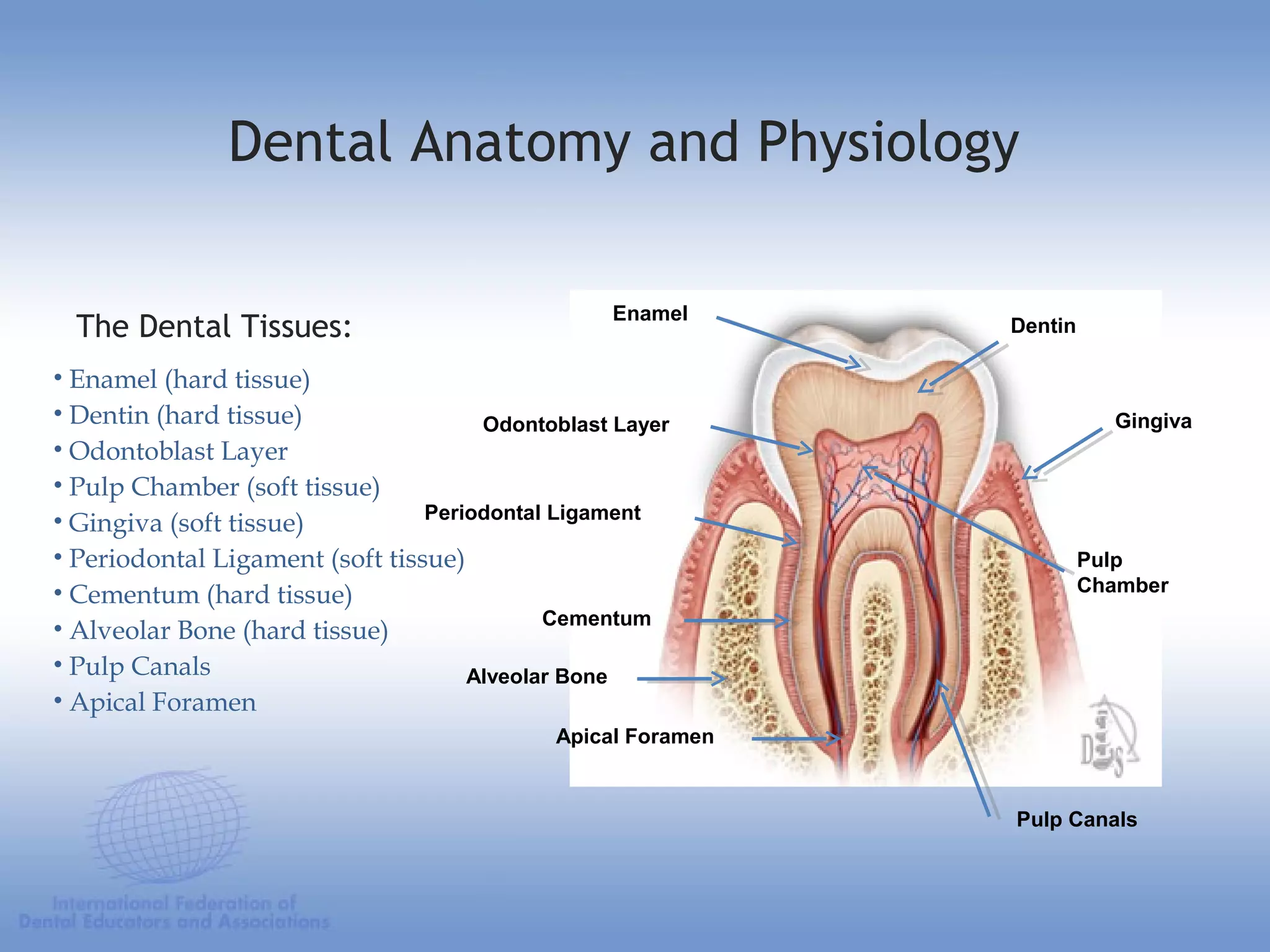




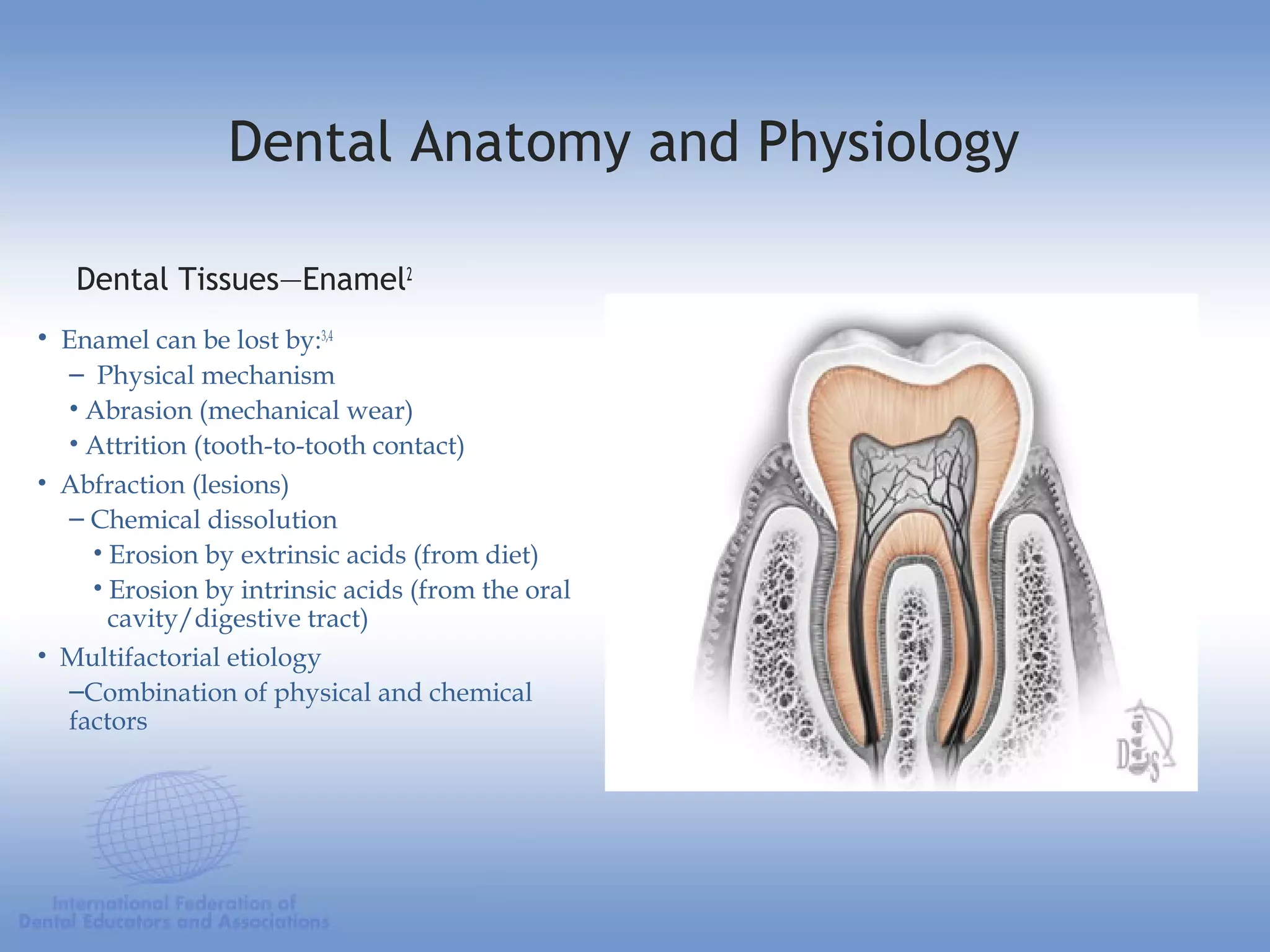













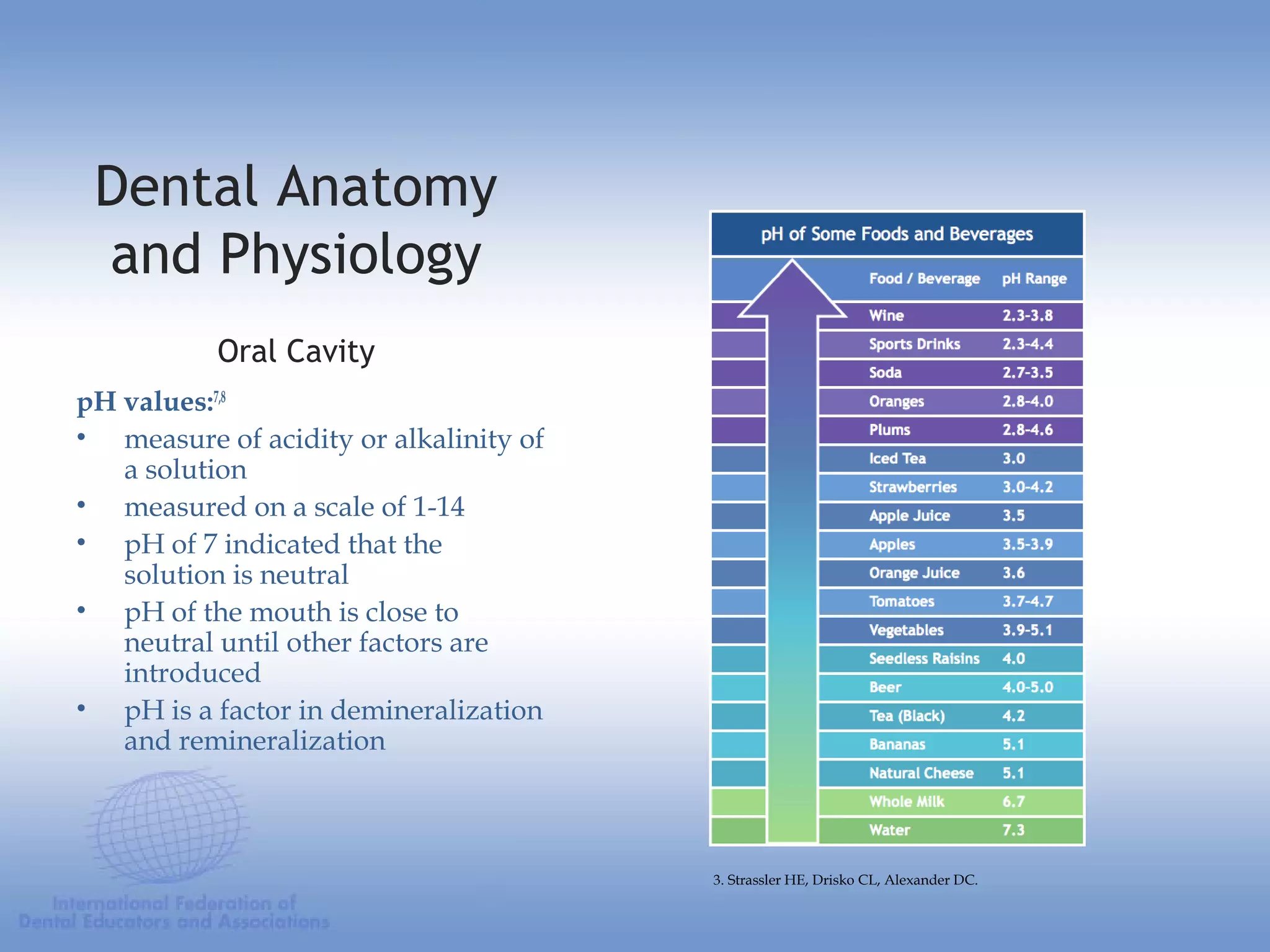





This document provides an overview of dental anatomy and physiology. It discusses the structures of teeth including enamel, dentin, cementum and dental pulp. It describes the primary and secondary dentitions. The document outlines the classification of teeth as incisors, canines, premolars and molars. It also discusses the oral cavity environment including plaque, saliva, pH values as they relate to demineralization and remineralization.























































































