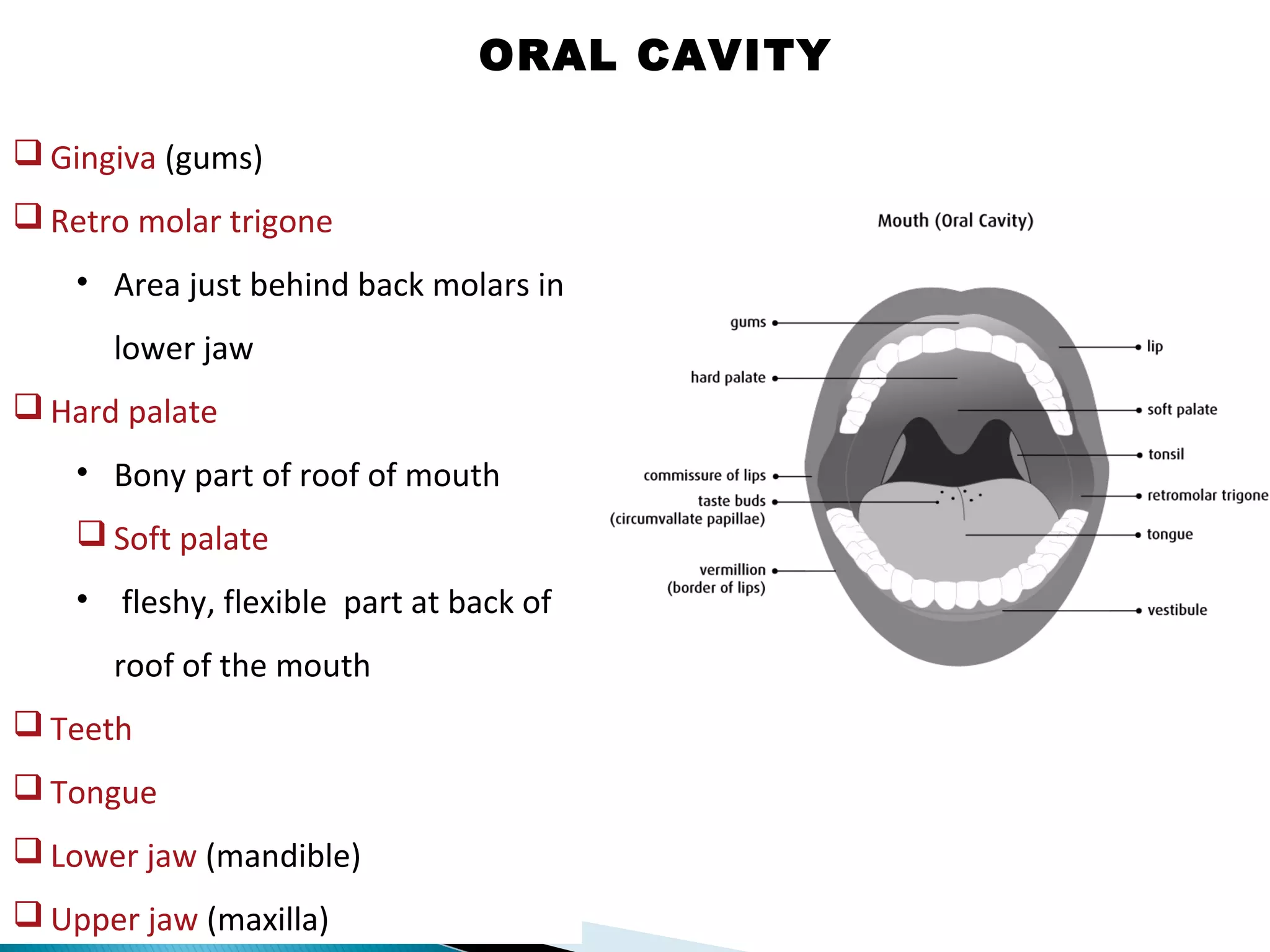
![Oral cavity includes:
Lips
Commissure of lips :
• Where upper & lower lips
meet at corner of mouth.
Vestibule :
• Space bounded by teeth,
gums, Mucosal surface of the
lips & cheeks [on both sides].
Buccal mucosa :
• Inner lining of cheeks
ORAL CAVITY](https://image.slidesharecdn.com/dentalanatomyphysiology-190107062108/75/Dental-anatomy-amp-physiology-3-2048.jpg)
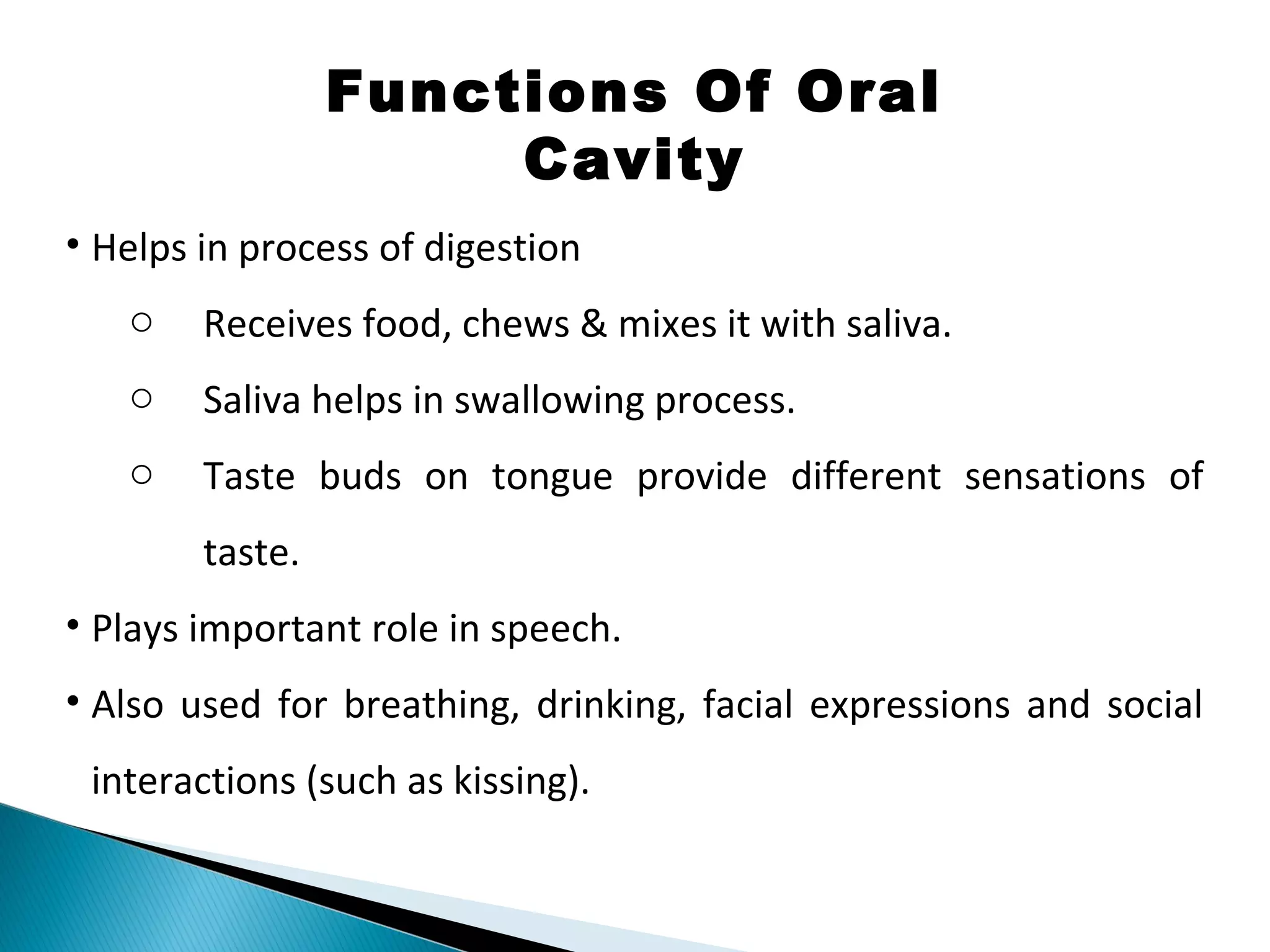

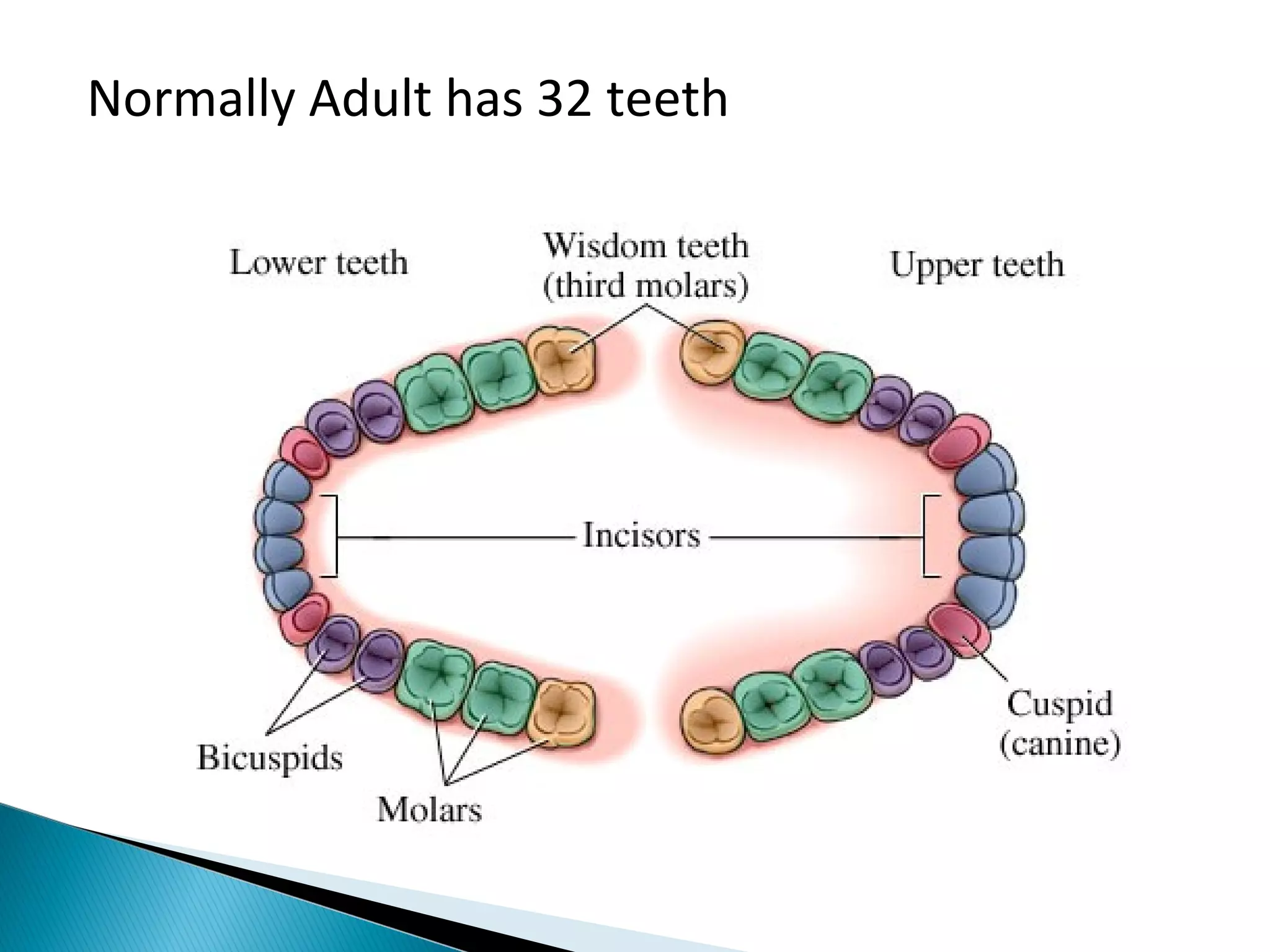
![Incisor Canine Premolar Molar
7
Incisors - Cut food
Canines - Shred [scrap or cut] food
Premolars - Chew & grind food
Molars - Grinding food
Mandible
Maxilla Incisors
Canine
Premolars
Molars](https://image.slidesharecdn.com/dentalanatomyphysiology-190107062108/75/Dental-anatomy-amp-physiology-7-2048.jpg)





!["Demineralization" – means "dissolution of enamel.“
Substantial number of mineral ions may get removed from
Hydroxyapatite [HAP] latticework without destroying its structural
integrity.](https://image.slidesharecdn.com/dentalanatomyphysiology-190107062108/75/Dental-anatomy-amp-physiology-23-2048.jpg)
![How does Demineralization
happen?
At pH ≤ 4.5, HAP can get
dissolved in process known as
demineralisation.
More the acidic
environment, greater is the
outward flow [loss] of ions.
Demineralization phase if
continues for longer period,
may cause excessive loss of
minerals, leading to loss of
enamel structure.
J Conserv Dent. 2016 Jul-Aug; 19(4): 328–331.
International Journal of Advanced Health Sciences 2015; 1(10): 21-
24](https://image.slidesharecdn.com/dentalanatomyphysiology-190107062108/75/Dental-anatomy-amp-physiology-24-2048.jpg)

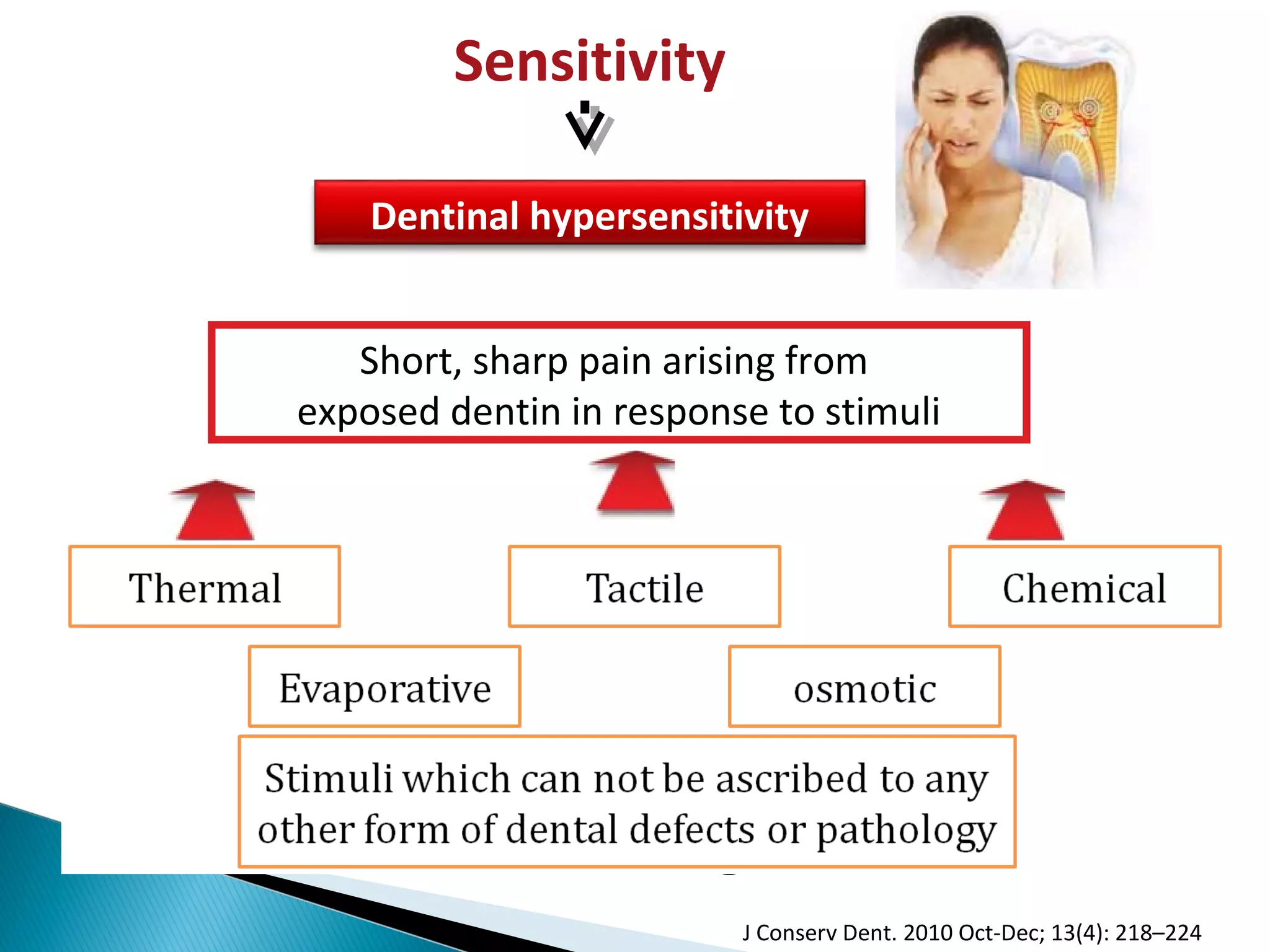
![Dental hypersensitivity:
Etiology
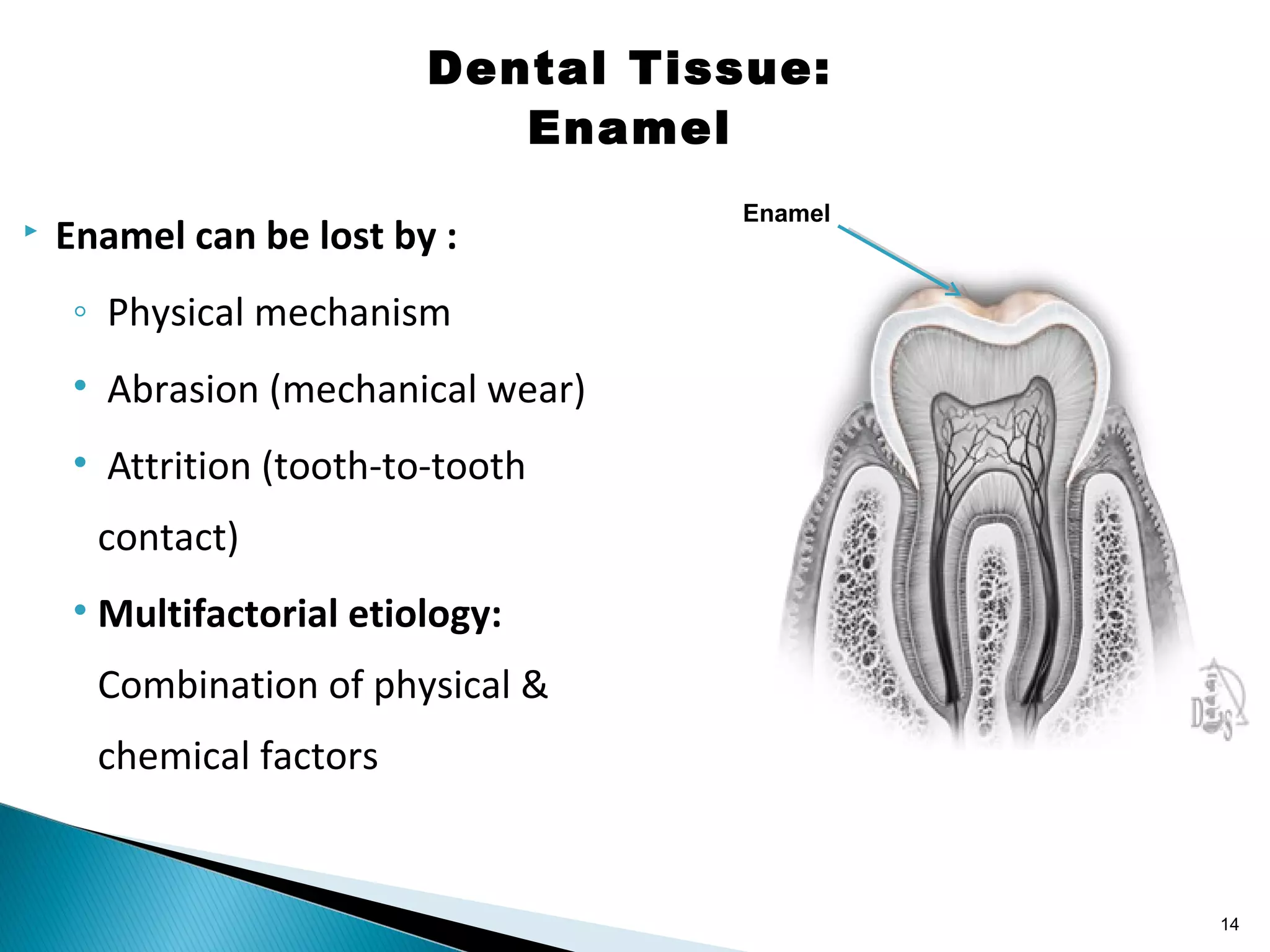
Loss of enamel
[wear]
Loss of
Cementum
Loss of gingival
tissue
Exposed
Dentin
Dental
hypersensitivity](https://image.slidesharecdn.com/dentalanatomyphysiology-190107062108/75/Dental-anatomy-amp-physiology-27-2048.jpg)
![Normal Vs. Sensitive teeth
Loss of enamel
[wear]
Loss of gingival
tissue
Loss of
Cementum
Exposed
Dentin](https://image.slidesharecdn.com/dentalanatomyphysiology-190107062108/75/Dental-anatomy-amp-physiology-28-2048.jpg)
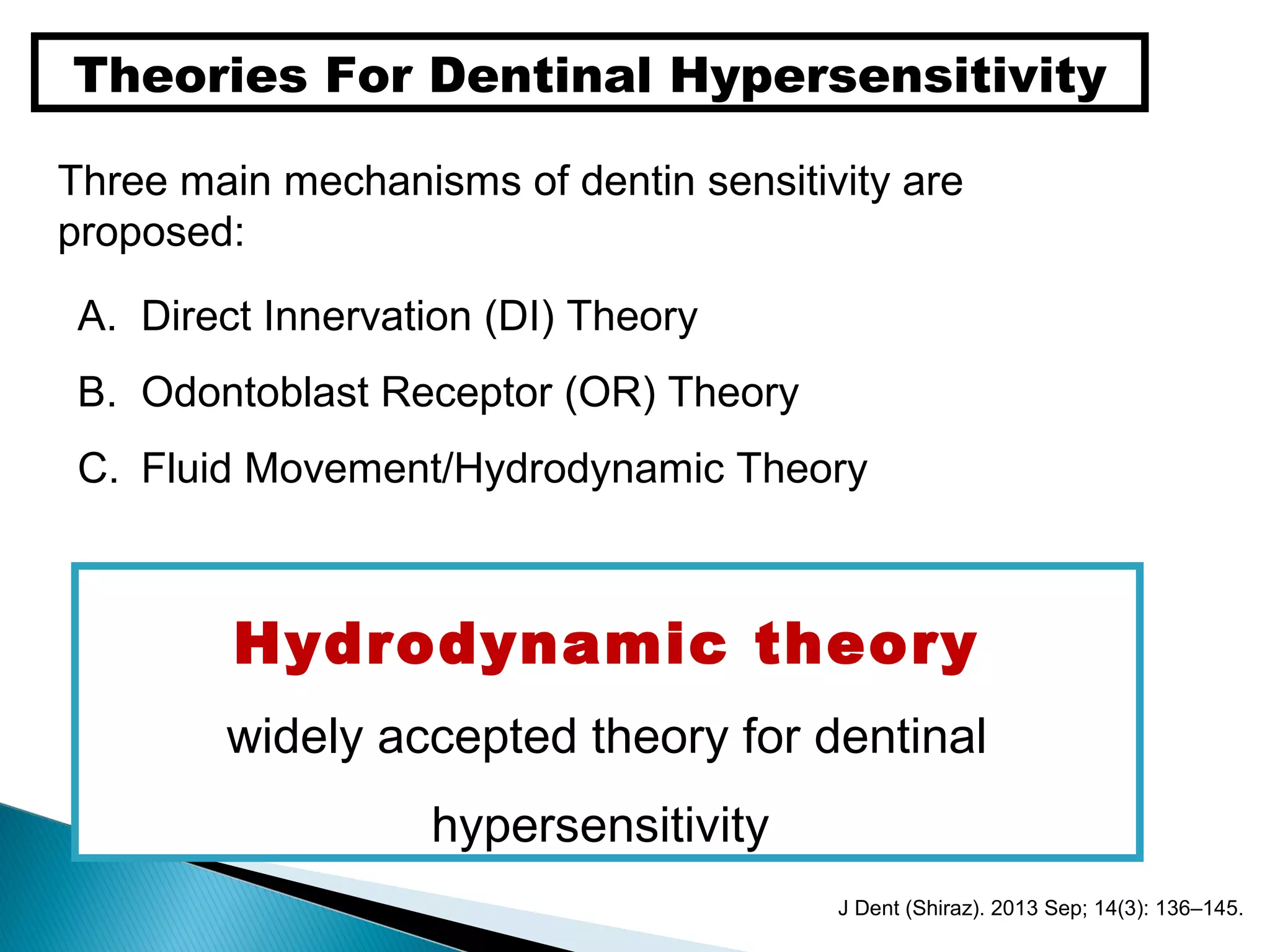



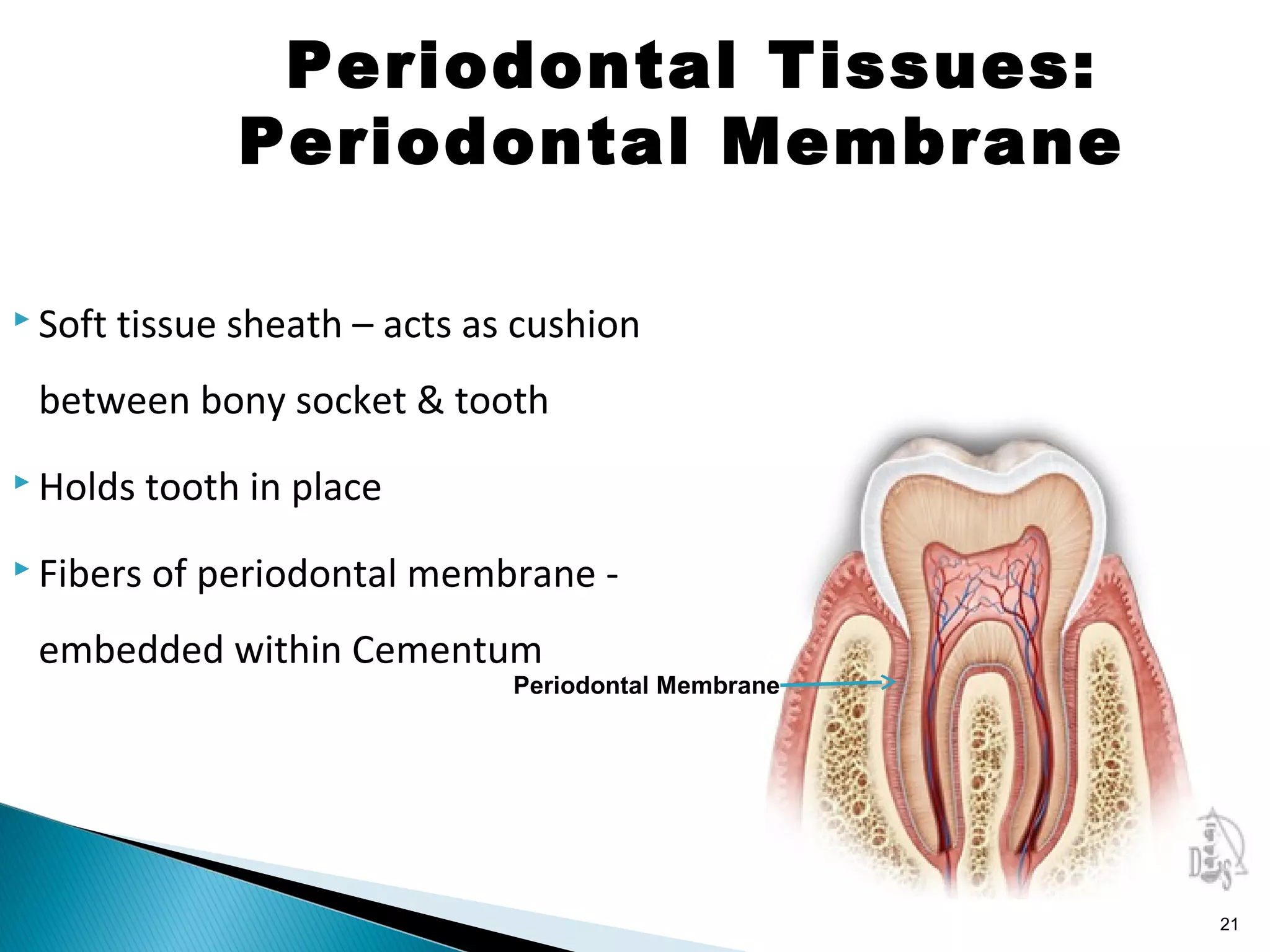
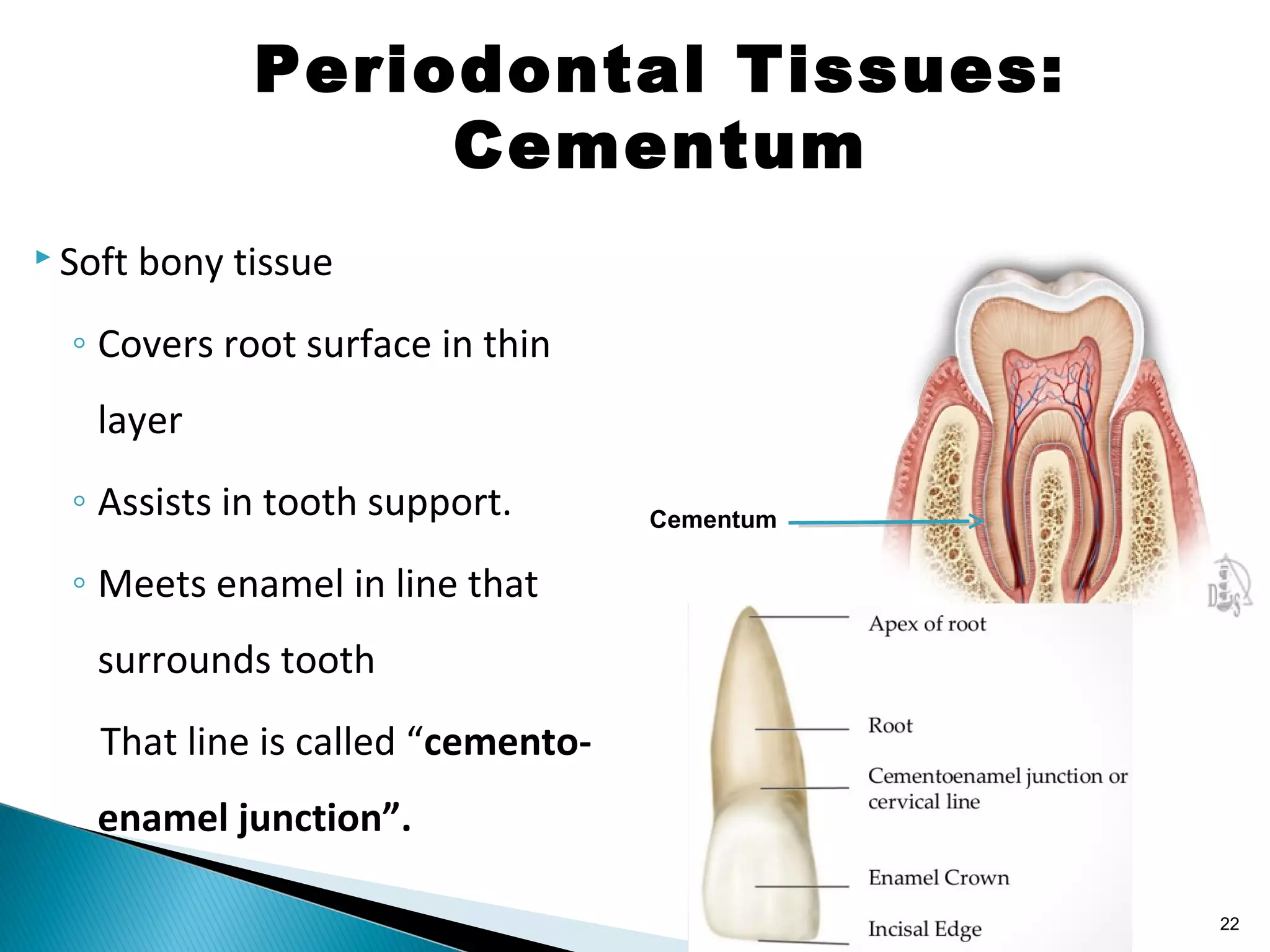
This document provides an overview of dental anatomy and physiology. It begins with an index of topics and then defines structures of the oral cavity such as the lips, gingiva, hard and soft palate, teeth, and tongue. Next, it describes the functions of the oral cavity in digestion, speech, and other roles. The document then discusses teeth anatomy and types, as well as the main dental tissues of enamel, dentin, and dental pulp. It also covers the periodontal tissues of gingiva, alveolar bone, cementum, and periodontal membrane. Finally, it briefly explains the processes of demineralization, remineralization, and theories of dentin sensitivity.










































































