Download to read offline
![INTRODUCTION
Vascularized tissue transfers have become
increasingly popular since the first description by
Seidenberg et al. in 1959 and currently plays an im-
portant role in reconstructive surgery centers (Urken
et al., 1991; Minami et al., 1992; Wilson et al.,
1998; Foster et al., 1999; Lyons et al., 2005; David
and Schmidt, 2008; Cannon et al., 2012). A consid-
erable number of flaps have since been evolved for a
multitude of indications (Baker and Sullivan, 1988;
Hidalgo, 1989; Hsu et al., 2007). The prerequisite
for the popularity of a flap are easy harvest, a high
success rate with minimal donor site morbidity, and
the prospect of a good functional and aesthetic out-
come (Taylor, 1982).
Incessant anatomical examinations and clinical
observations will improve successful application
flaps, limit donor site morbidity, while achieving the
desired outcome (Berggren et al., 1982; Ramasastry
et al., 1986; Safak et al., 1997; Kimata et al., 2001;
Seikaly et al., 2003; Hsu et al., 2007). In addition
this will also reduce the operating time, which is
especially important in patients with poor medical
conditions (Berggren et al., 1982; August et al.,
2000; Cannon et al., 2012).
The vascularized iliac bone graft or deep circum-
flex iliac artery flap (DCIA) is unquestionably an
excellent source for replacement many different
parts of the facial bone structure (Riediger, 1988;
Uschida and Sugioka, 1990; Frodel et al., 1993; Sei-
kaly et al., 2003; Lyons et al., 2005). McGregor and
Jackson initially introduced it as the groin flap based
on the superficial circumflex iliac vessel (McGregor
and Jackson, 1972). Daniel and Taylor reported the
first clinical use as a free flap (Daniel and Taylor,
1973). The first detailed guideline for harvesting the
DCIA-flap along with several variations of the nour-
ishing vessels was described by Taylor and his group
(Taylor et al., 1979). Other authors have contributed
anatomical variations since then and have suggested
modifications to reduce donor site morbidity and
increase functional and aesthetic outcome (Rama-
sastry et al., 1986; Safak et al., 1997; Thein et al.,
1997; Winter and Smeele, 2000; Kimata et al.,
2001; Koshima et al., 2004; Hsu et al. 2007).
An extensive anatomical review of this region was
stimulated by the fact that many clinical variations
were described in the past by several authors but
none of them were complete. We therefore performed
an extensive examination of the DCIA and its relation-
ship to neighboring structures, with the aim of facili-
tating flap harvesting and improving the success rate.
MATERIALS AND METHODS
We performed bilateral anatomical dissections of
the iliac regions in 78 cadavers (n ¼ 156), 36
females and 42 males, with an average age of 76
years (age range 61–93 years). The anatomical find-
ings of 60 clinical cases, 24 females and 36 males,
with average age of 53 years (age range 12–84
years) were included. Altogether, we assessed 216
iliac regions. We documented the branching pat-
terns, diameters and the distances of the deep cir-
cumflex iliac artery (DCIA), the deep circumflex iliac
vein (DCIV), the superficial circumflex iliac artery
(SCIA), and the superficial circumflex iliac vein
(SCIV) to the following surgical landmarks (Fig. 1):
Inferior epigastric artery (IEA)
Anterior superior iliac spine (ASIS)
Bifurcation of femoral artery (FA)
Inguinal ligament (IL)
The cadaver dissections were performed by three
examiners. We proposed a modification of the avail-
able classification of the deep and superficial circum-
flex iliac vessels for easier orientation. All findings
were recorded photographically and clear illustra-
tions were made for each variation (Figs. 2–16).
Data were collected in a table using Microsoft Excel
(version 2010, Microsoft, Redmond, WA), and the
data were filtered according to all eligible target pa-
rameters for the subsequent descriptive analysis
that was performed with SPSS 14 under Windows XP
(SPSS, Chicago, IL).
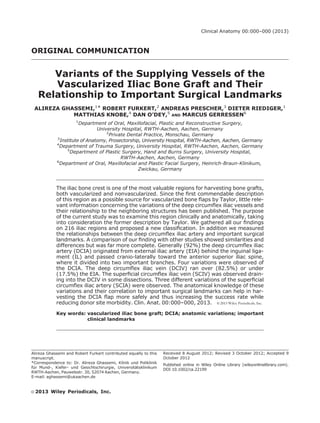
Fig. 1. Relationship between the DCIA and impor-
tant clinical landmarks. A: Distance from the origin of
the DCIA to the ASIS. B: Distance from the origin of the
DCIA to the origin of the AB. C: Distance from the origin
of the DCIA to the division of the AF. D: Distance from
the IL to the division of the AF. E: Diameter of the DCIA
directly after leaving the EIA. F: Relation between the
origins of the DCIA and the IEA. G: Distance from the
origin of the DCIA to the origin of the SCIA. H: Distance
from the ASIS to the crossing point of the HB with the
iliac crest. I: Vertical distance from the HB to the ASIS.
[Color figure can be viewed in the online issue, which is
available at wileyonlinelibrary.com.]
2 Ghassemi et al.](https://image.slidesharecdn.com/2013-ghassemi-dciavariantsclan-190613143739/85/2013-ghassemi-dcia-variants-clan-2-320.jpg)
![RESULTS
The DCIA had a diameter of 1.5–3 mm (average
2.51 mm) and originated laterally or postero-laterally
from the EIA behind the IL. Its origin was mostly adja-
cent (50%), slightly proximal (44%) or distal (6%)
from the IEA. The IEA could also be used as an intrao-
perative guide to find the DCIA. It runs cranio-laterally
Fig. 2. (a,b) Subtype Ia showing equal HB and AB. [Color figure can be
viewed in the online issue, which is available at wileyonlinelibrary.com.]
Fig. 3. (a,b) Subtype Ib showing two or more HB. [Color figure can be
viewed in the online issue, which is available at wileyonlinelibrary.com.]
3Anatomy and Topography of DCIA Flap](https://image.slidesharecdn.com/2013-ghassemi-dciavariantsclan-190613143739/85/2013-ghassemi-dcia-variants-clan-3-320.jpg)
![Fig. 4. (a,b) Subtype Ic with later branching of the AB. [Color figure can
be viewed in the online issue, which is available at wileyonlinelibrary.com.]
Fig. 5. (a,b) Subtype Id with dominant AB. [Color figure can be viewed in
the online issue, which is available at wileyonlinelibrary.com.]
4 Ghassemi et al.](https://image.slidesharecdn.com/2013-ghassemi-dciavariantsclan-190613143739/85/2013-ghassemi-dcia-variants-clan-4-320.jpg)
![Fig. 6. (a,b) Subtype Ie with no AB, but multiple small branches. [Color figure
can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
Fig. 7. (a,b) Type II with a short common trunk of the HB and the AB. [Color fig-
ure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
5Anatomy and Topography of DCIA Flap](https://image.slidesharecdn.com/2013-ghassemi-dciavariantsclan-190613143739/85/2013-ghassemi-dcia-variants-clan-5-320.jpg)
![along and posteriorly to the IL towards the ASIS and
reaches the iliac medial aspect after 4.9–10.8 cm (av-
erage 7.06 cm), where it divides into two main
branches, the horizontal (HB) and the ascending
branch (AB). The HB then runs 0.5–2.5 cm (average
1.40 cm) medially below the ASIS on the iliacus muscle
dorso-cranially and crosses the iliac crest after 3–7.5
cm (average 5.79 cm). The HB gives of several perfo-
rators to the skin and bone and eventually anastomo-
ses with the iliolumbal vessel posteriorly (Fig. 17). The
AB leaves the main vessel after 0–12 cm (average
2.69 cm) from its origin. It runs medio-cranially toward
the transverse and internal oblique muscle. The dis-
tance from the origin of the DCIA to the origin of SCIA
from the femoral artery measured 0–4.5 cm (average
1.94 cm). The distance to the bifurcation of the femoral
artery was from 2.5 to 9 cm (average 4.56 cm). The
results of the data are summarized in Table 1.
The observed variations of the DCIA, the SCIA,
and the accompanying veins were as follows:
Four Main DCIA Variations
Type I showed four different variations and was
observed in 199 (92%) dissections. The four differ-
ent variations or subdivisions were named sub-type
Ia, Ib, Ic, Id, and Ie (Figs. 2a and 2b, 3a and 3b, 4a
and 4b, 5a and 5b, and 6a and 6b).
The next variation, which we named Type II,
showed a very short common trunk of the HB and
the AB and was observed in 9 (4.2%) dissections
(Figs. 7a and 7b).
In 6 (2.8%) dissections we observed a separate
origin of the HB and the AB from the EIA, which we
categorized as Type III (Figs. 8a and 8b), and in two
dissections (1%) we saw a common origin of the IEA
and the DCIA from the EIA and was named Type IV
(Figs. 9a and 9b).
Three Main SCIA Variations
In 179 (83%) dissections the SCIA originated
below the IL and had either one (Figs. 2a and 10)
or two branches Figs. 11a and 11b). This was
named the Type I SCIA variation. In 25 (11.5%)
dissections the SCIA originated from the DCIA,
which we named Type II (Figs. 12a and 12b).
Finally in 12 (5.5%) dissections we could not
find any SCIA and thus categorized it as Type III
(Figs. 13a and 13b).
Three Main DCIV Variations
The accompanying veins of the DCIA unite shortly
before draining into the external iliac vein (EIV) near
the arterial origin, which then runs slightly upward to
cross over (Type I) (male 75%, female 87.5%) or
below (Type II) (male 25%, female 12.5%) the EIA
to drain into the external iliac vein (EIV) (Figs. 14a
and 14b and 15a and 15b). in some cases the DCIV
anastomoses with the SCIV before forming a com-
mon trunk and was categorized as Type III (Figs.
16a and 16b).
Fig. 8. (a,b) Type III with separate origin of the HB and the AB from the EIA. [Color figure can be viewed in
the online issue, which is available at wileyonlinelibrary.com.]
6 Ghassemi et al.](https://image.slidesharecdn.com/2013-ghassemi-dciavariantsclan-190613143739/85/2013-ghassemi-dcia-variants-clan-6-320.jpg)
![DISCUSSION
The iliac region not only offers favorable bone
quality, but also excellent bone quantity. This makes
the DCIA flap appropriate for the reconstruction of
different parts of the facial skeleton, especially the
load bearing structures, such as the mandible, or
complex structures like the zygoma (Riediger, 1988;
Frodel et al., 1993; Seikaly et al., 2003; Modabber
et al., 2012). Many factors contribute to the success-
ful transfer of a vascularized iliac bone graft, and its
harvesting can be very challenging (Berggren et al.,
1982; Taylor, 1982; Urken, 1991; August, 2000).
The difficult anatomy and donor site morbidity follow-
ing flap harvest play an important role when choosing
the DCIA (Jewer et al., 1988). During our long clinical
experience in using this vascularized bone graft, we
encountered several variations that were not clearly
described in the literature. It stimulated us to this
extensive anatomical study. The awareness of these
variations in anatomy and the knowledge of exact
clinical landmarks are essential to reducing flap fail-
ure and donor site morbidity (Ghassemi et al., 2009,
2012). The absence of a clear and complete map of
the iliac region may be the reason for it being less
popular as compared to the vascularized fibular flap
over the past two decades. The vascularized fibular
flap however does not always offer sufficient bone
material and often requires an additional procedure
(Schleier et al., 2006).
The DCIA was vaguely described in 1892, when
Stieda from Ko¨nigsberg published his remarkable
study searching for the cause of bleeding when
puncturing the abdominal wall (Stieda, 1892). He
called this vessel the lateral epigastric artery. In
1928, Adachi described the DCIA very adequately in
Japanese. However, the clinical importance of the
SCIA and the DCIA was later clearly illustrated as
the main supplying vessel of the bone flap by Taylor
in his excellent experimental and clinical work
Fig. 9. (a,b) Type IV, a common origin of the DCIA
and IEA from the EIA. [Color figure can be viewed in the
online issue, which is available at wileyonlinelibrary.
com.]
Fig. 10. Classic type Ia originates below the IL
from the FA. [Color figure can be viewed in the online
issue, which is available at wileyonlinelibrary.com.]
7Anatomy and Topography of DCIA Flap](https://image.slidesharecdn.com/2013-ghassemi-dciavariantsclan-190613143739/85/2013-ghassemi-dcia-variants-clan-7-320.jpg)
![Fig. 11. (a,b) Variant type Ib showing two branches of the SCIA. [Color figure
can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
Fig. 12. (a,b) Variant type II originates from the DCIA. [Color figure can
be viewed in the online issue, which is available at wileyonlinelibrary.com.]
8 Ghassemi et al.](https://image.slidesharecdn.com/2013-ghassemi-dciavariantsclan-190613143739/85/2013-ghassemi-dcia-variants-clan-8-320.jpg)
![Fig. 13. (a,b) Variant type III, where no SCIA is seen. [Color figure can
be viewed in the online issue, which is available at wileyonlinelibrary.com.]
Fig. 14. (a,b) Type I, which crosses over the EIA. [Color figure can be
viewed in the online issue, which is available at wileyonlinelibrary.com.]
9Anatomy and Topography of DCIA Flap](https://image.slidesharecdn.com/2013-ghassemi-dciavariantsclan-190613143739/85/2013-ghassemi-dcia-variants-clan-9-320.jpg)
![Fig. 15. (a,b) Type II, which crosses below the EIA. [Color figure can be
viewed in the online issue, which is available at wileyonlinelibrary.com.]
Fig. 16. (a,b) Type III, which anastomoses with the SCIV. [Color figure can
be viewed in the online issue, which is available at wileyonlinelibrary.com.]
10 Ghassemi et al.](https://image.slidesharecdn.com/2013-ghassemi-dciavariantsclan-190613143739/85/2013-ghassemi-dcia-variants-clan-10-320.jpg)
![(Taylor et al., 1979). He also mentioned many varia-
tions that are still relevant in flap elevation. How-
ever, our findings presented in Table 2 are more
extensive and complete when compared to all former
descriptions of this region.
In some dissections the ascending branch was
absent or we observed many small side branches, as
similarly reported by Taylor (Taylor et al., 1979), Bit-
ter (Bitter and Danai, 1983) and Thein (Thein et al.,
1999). This is essential when considering harvesting
the DCIA along with the oblique iliac muscle for addi-
tional soft tissue coverage. In two cases we found
the DCIA originating from the inferior epigastric ar-
tery, which to our knowledge was previously only
vaguely described by Adachi (Figs. 9a and 9b).
Taylor stated that the DCIV passed beneath the
EIA in half of the cases he studied. In our series we
inspected about 75% (male) and up to 87.5%
(female) cases, in which the vein over-crossed (Figs.
14a and 14b) the EIA, and only in 25% (male) or
12.5% (female) the vein under-crossed the EIA
(Figs. 15a and 15b). In 103 (48%) dissections we
observed a connection of the DCIA with the SCIV
(Figs. 16a and 16b). Furthermore, the variations of
the SCIA are of extreme importance when consider-
ing inclusion in flap elevation. In about 17% (n ¼ 37)
of dissections we could not find any SCIA, or it origi-
nated from the DCIA.
Thein et al. (1999) were able to find some of
these variations and emphasized the course of the
horizontal branch in relation to the ASIS. To reduce
donor site morbidity, they suggested bone harvest
beneath the iliac crest to maintain the stability and
contour of the iliac bone. Our measurement illus-
trated a distance of 0.5–2.5 cm (average 1.40 cm)
of the DCIA to the iliac crest, which clearly opposes
this recommendation. Leaving the iliac spine or iliac
crest could jeopardize the nourishing vessel of the
bone. Besides, we have been performing the har-
vesting of the iliac ASIS and the iliac crest for years
without major complications (Ghassemi et al., 2009,
2012).
The perforators to the skin that originated from the
HB were visible in all examined iliac regions and had
varying diameters. As a rule the last perforator that is
actually the continuation of the HB, is the largest per-
forator supplying the skin (Figs. 2b, 4b, 7b, and 12b).
This perforator crosses the iliac crest at a distance of
3–7.5 cm from the ASIS. It also branches of to the ilio-
lumbal vessel of the internal iliac artery (Safak et al.,
1997; Kimata et al., 2001; Koshimata et al., 2004)
(Fig. 17). The lateral femoral subcutaneous nerve,
which crosses the DCIA and can be injured while har-
vesting the flap, has been thoroughly examined
(Doklamyai et al., 2008; Carai et al., 2009).
The vascularized iliac bone flap, despite many
advantages, is burdened by a series of drawbacks
Fig. 17. Anastomsis of the HB of DCIA with iliolum-
bal vessel. [Color figure can be viewed in the online
issue, which is available at wileyonlinelibrary.com.]
TABLE 1. Measurement of Relevant Landmarks
A (cm) B (cm) C (cm) D (cm) E (mm) G (cm) H (cm) I (cm)
Max 10.8 12 9 9 1.5 4.5 7.5 2.5
Min 4.9 0 2.5 2 3 0 3 0.5
Mean 7.03 2.69 4.56 4.25 2.51 1.94 5.79 1.40
A: Distance from the origin of the DCIA to the ASIS.
B: Distance from the origin of the DCIA to the origin of the ascending branch.
C: Distance from the origin of the DCIA to the division of the AF.
D: Distance from the IL to the division of the AF.
E: Diameter of the DCIA directly after leaving the EIA.
G: Distance from the origin of the DCIA to the origin of the SCIA.
H: Distance from the ASIS to the crossing point of the horizontal branch with the iliac crest.
I: Vertical distance from the HB to the ASIS.
11Anatomy and Topography of DCIA Flap](https://image.slidesharecdn.com/2013-ghassemi-dciavariantsclan-190613143739/85/2013-ghassemi-dcia-variants-clan-11-320.jpg)
![that could be explained by the technically difficult
harvest. Several prerequisites have emerged for a
successful flap transfer. The anatomy of the flap and
the steps for its elevation should be well understood.
It will help the operating surgeon to protect the im-
portant structures during flap elevation. This study is
based on cadaver dissection along with clinical case
observations. The variations presented can cause
difficult surgical challenges. Our intention was to
present the relevant anatomical variations of the
vascularized iliac bone graft in considerable detail.
We could confirm some findings of other authors,
however they lacked a complete overview and we
additionally established a new practical classification.
The relationship between the feeding vessels of the
DCIA flap and important and relevant clinical land-
marks is presented here in detail and should enable
a safer guide to harvest this flap.
REFERENCES
Adachi B. 1928. The Arterial System of the Japanese. Vol II.
Koyoto: Imperial Japanese University of Koyoto. p 132–136.
August M, Tompach P, Chang Y, Kaban L. 2000. Factors influencing
the long-term outcome of mandibular reconstruction. J Oral
Maxillofac Surg 58:731–738.
Baker SR, Sullivan MJ. 1988. Osteocutaneous free scapular flap for
one-stage mandibular reconstruction. Arch Otolaryngol Head
Neck Surg 114:267–277.
Berggren A, Weiland AJ, Dorfman H. 1982. Free vascularized bone
grafts: Factors affecting their survival and ability to heal to re-
cipient bone defects. Plast Reconstr Surg 69:19–29.
Bitter K, Danai T. 1983. The iliac bone or osteocutaneous transplant
pedicled to the deep circumflex Iliac artery. I. Anatomical and
technical considerations. J Maxillofac Surg 11:195–200.
Cannon TY, Strub GM, Yawn RJ, Day TA. 2012. Oromandibular
reconstruction. Clin Anat 25:108–119.
Carai A, Fenu G, Sechi E, Crotti FM, Montella A. 2009. Anatomical
variability of the lateral femoral cutaneous nerve: Findings from
a surgical series. Clin Anat 22:365–370.
Daniel RK, Taylor GI. 1973. Distant transfer of an island flap by mi-
crovascular anastomoses. A clinical technique. Plast Reconstr
Surg 52:111–117.
Doklamyai P, Agthong S, Chentanez V, Huanmanop T, Amarase C,
Surunchupakorn P, Yotnuengnit P. 2008. Anatomy of the lateral
femoral cutaneous nerve related to inguinal ligament, adjacent
bony landmarks, and femoral artery. Clin Anat 21:769–774.
Foster RD, Anthony JP, Sharma A, Pogrel MA. 1999. Vascularized
bone flaps versus nonvascularized bone grafts for mandibular
reconstruction: An outcome analysis of primary bony union and
endosseous implant success. Head Neck 21:66–71.
Frodel JL Jr, Funk GF, Capper DT, Fridrich KL, Blumer JR, Haller JR,
Hoffman HT. 1993. Osseointegrated implants: A comparative
study of bone thickness in four vascularized bone flaps. Plast
Reconstr Surg 92:449–458.
Ghassemi A, Ghassemi M, Riediger D, Hilgers RD, Gerressen M.
2009. Comparison of donor-site engraftment after harvesting
vascularized and nonvascularized iliac bone grafts. J Oral Maxil-
lofac Surg 67:1589–1594.
Ghassemi A, Ghassemi M, Modabber A, Knobe M, Fritz U, Riediger
D, Gerressen M. 2012. Functional long-term results after the
harvest of vascularized iliac bone grafts bicortically with the an-
terior superior iliac spine included. Br J Oral Maxillofac Surg.
2012 Jun 5 [Epub ahead of print].
Hidalgo DA. 1989. Fibula free flap: A new method of mandible
reconstruction. Plast Reconstr Surg 84:71–79.
Hsu WM, Chao WN, Yang C, Fang CL, Huang KF, Lin YS, Lee TH.
2007. Evolution of the free groin flap: The superficial circumflex
iliac artery perforator flap. Plast Reconstr Surg 15:1491–1498.
Jewer DD, Boyd JB, Manktelow RT, Zuker RM, Rosen IB, Gullane PJ,
Rotsteinund LE, Freeman JE. 1989. Orofacial and mandibular recon-
struction with the iliac crest free flap: A review of 60 cases and a
new method of classification. Plast Reconstr Surg 84:391–405.
Kimata Y, Uchiyama K, Sakuraba M, Ebihara S, Hayashi R, Asakage
T, Nakatsuka T, Harii K. 2001. Deep circumflex iliac perforator
flap with iliac crest for mandibular reconstruction. Br J Plast Surg
54:487–490.
Koshima I, Nanba Y, Tsutsui T, Itoh S. 2004. Sequential vascular-
ized Ilac bone graft and a superficial circumflex Iliac artery per-
forator flap with a single source vessel for established mandibu-
lar defects. Plast Reconstr Surg 113:101–106.
Lyons AJ, James R, Collyer J. 2005. Free vascularized iliac crest
graft: An audit of 26 consecutive cases. Br J Oral Maxillofac Surg
43:210–214.
McGregor IA, Jackson IT. 1972. The groin flap. Br J Plast Surg
25:3–16.
Minami A, Kaneda K, Itoga H. 1992. Treatment of infected segmen-
tal defect of long bone with vascularized bone transfer. J
Reconstr Microsurg 8:75–82.
Modabber A, Gerressen M, Stiller M, Noroozi N, Fu¨glein A, Ho¨lzle F,
Riediger D, Ghassemi A. 2012. Computer-assisted mandibular
reconstruction with vascularized Iliac crest bone graft. Aesthetic
Plast Surg 36:653–659.
Ramasastry SS, Granick MS, Futrell JW. 1986. Clinical anatomy of
the internal oblique muscle. J Reconstr Microsurg 2:117–122.
Riediger D. 1988. Restoration of masticatory function by microsurgi-
cally revascularized iliac crest bone grafts using enosseous
implants. Plast Reconstr Surg 81:861–877.
Safak T, Klebuc MJ, Mavili E, Shenaq SM. 1997. A new design of the
iliac crest microsurgical free flap without including the ‘‘obliga-
tory’’ muscle cuff. Plast Reconst Surg 100:1703–1709.
Schleier P, Hyckel P, Fried W, Beinemann J, Wurdinger J, Hinz M,
Steen M, Schumann D. 2006. Vertical distraction of fibula trans-
plant in a case of mandibular defect caused by shotgun injury.
Int J Oral Maxillofac Surg 35:861–864.
Seidenberg B, Rosenak SS, Hurwitt HS, Som ML. 1959. Immediate
reconstruction of the cervical esophagus by a revascularized iso-
lated jejunal segment. Ann Surg 149:162–171.
Seikaly H, Chau J, Li F, Driscoll B, Seikaly D, Calhoun J, Calhoun
KH. 2003. Bone that best matches the properties of the mandi-
ble. J Otolaryngol 32:262–265.
Stieda H. 1892. U¨ber die Arteria circumflexa ilium. Anat Verh
7:232–245.
Taylor GI. 1982. Reconstruction of the mandible with free composite
iliac bone grafts. Ann Plast Surg 9:361–376.
TABLE 2. Comparison of the Results of Different
Studies
Present
Study
Stieda
(1892)
Adachi
(1928)
Taylor
(1979)
Thein
(1997)
DCIA
Type I X X X X
Type Ia X X
Type Ib X X
Type Ic X X X
Type Id X X X X
Type II X X
Type III X X X X
Type IV X X
DCIV
Type I X X
Type II X X
Type III X X
SCIA
Type Ia X X X
Type Ib X X
Type II X X X
Type III X X
12 Ghassemi et al.](https://image.slidesharecdn.com/2013-ghassemi-dciavariantsclan-190613143739/85/2013-ghassemi-dcia-variants-clan-12-320.jpg)


This document describes a study examining variations in the anatomy of blood vessels that supply the iliac bone. The researchers dissected 216 iliac regions from cadavers and clinical cases. They observed four main variations in the origin and branching patterns of the deep circumflex iliac artery, which is the primary blood vessel supplying the iliac bone. The relationships between this artery and surrounding anatomical landmarks like the anterior superior iliac spine were also measured. Documenting these variations will help surgeons more safely harvest vascularized bone grafts from the iliac crest while reducing complications.



















































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)















