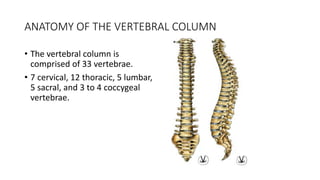
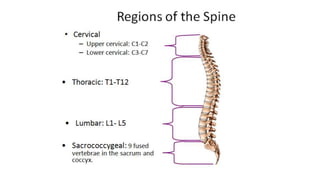
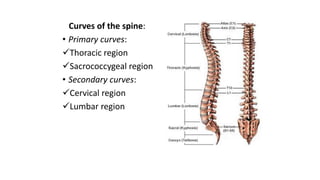
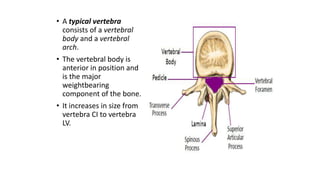
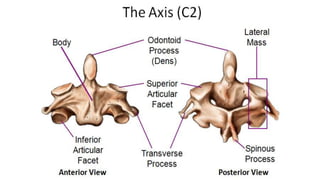
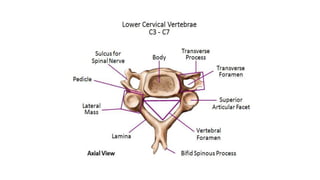
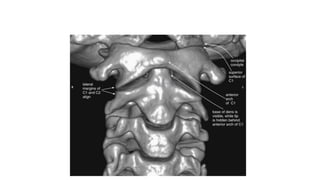
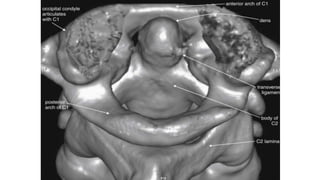
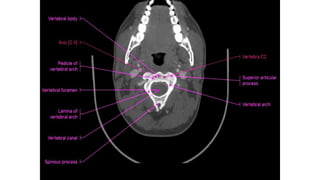
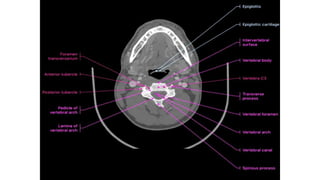
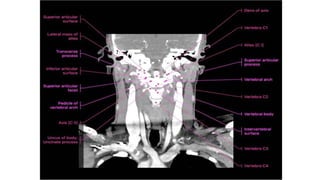
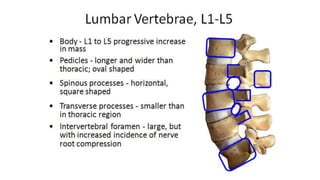
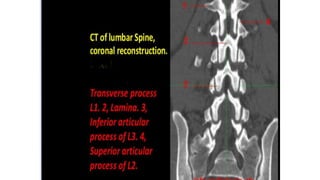
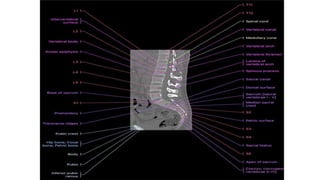
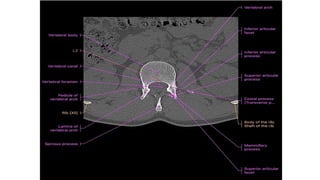
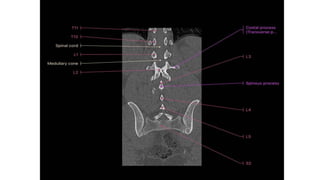
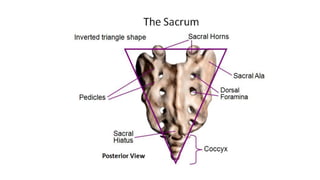
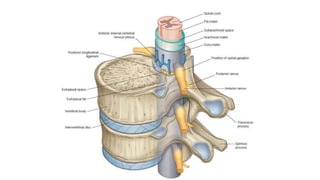
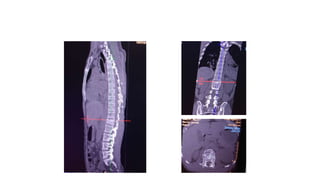
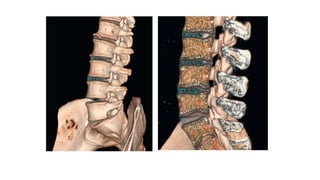
This document provides an overview of CT imaging of the cervical spine. It discusses the anatomy of the cervical spine including the typical vertebrae and curves. It describes the techniques used in CT imaging, including positioning the patient and acquiring scans to allow reconstruction in multiple planes. CT is useful for trauma evaluation and detecting fractures. Example images show normal anatomy on CT as well as a burst fracture. The document also provides some basics on lumbar spine and pelvis anatomy.