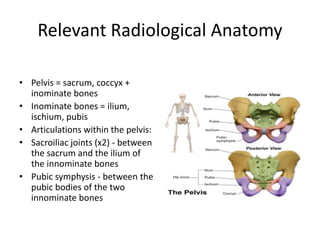
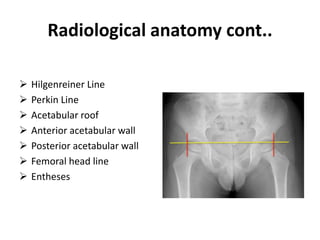
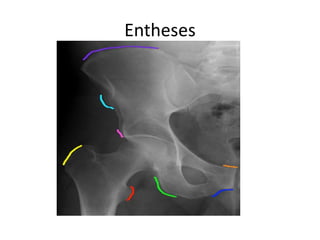
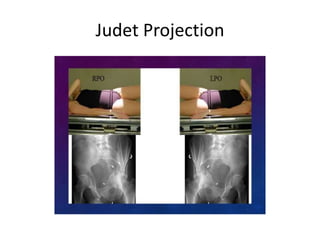
This document provides an overview of how to read pelvic and hip radiographs. It discusses the relevant radiological anatomy of the pelvis, including important bones, lines, and articulations. It describes common radiographic views used to image the hip and pelvis, such as AP, lateral, and Judet projections. It outlines how to systematically read a pelvic radiograph, including assessing adequacy, soft tissues, joint space, and bones. Examples of normal anatomy and pathological findings are shown, such as fractures, infections, and developmental dysplasia. The conclusion emphasizes understanding normal anatomy and disease patterns aids accurate diagnosis.