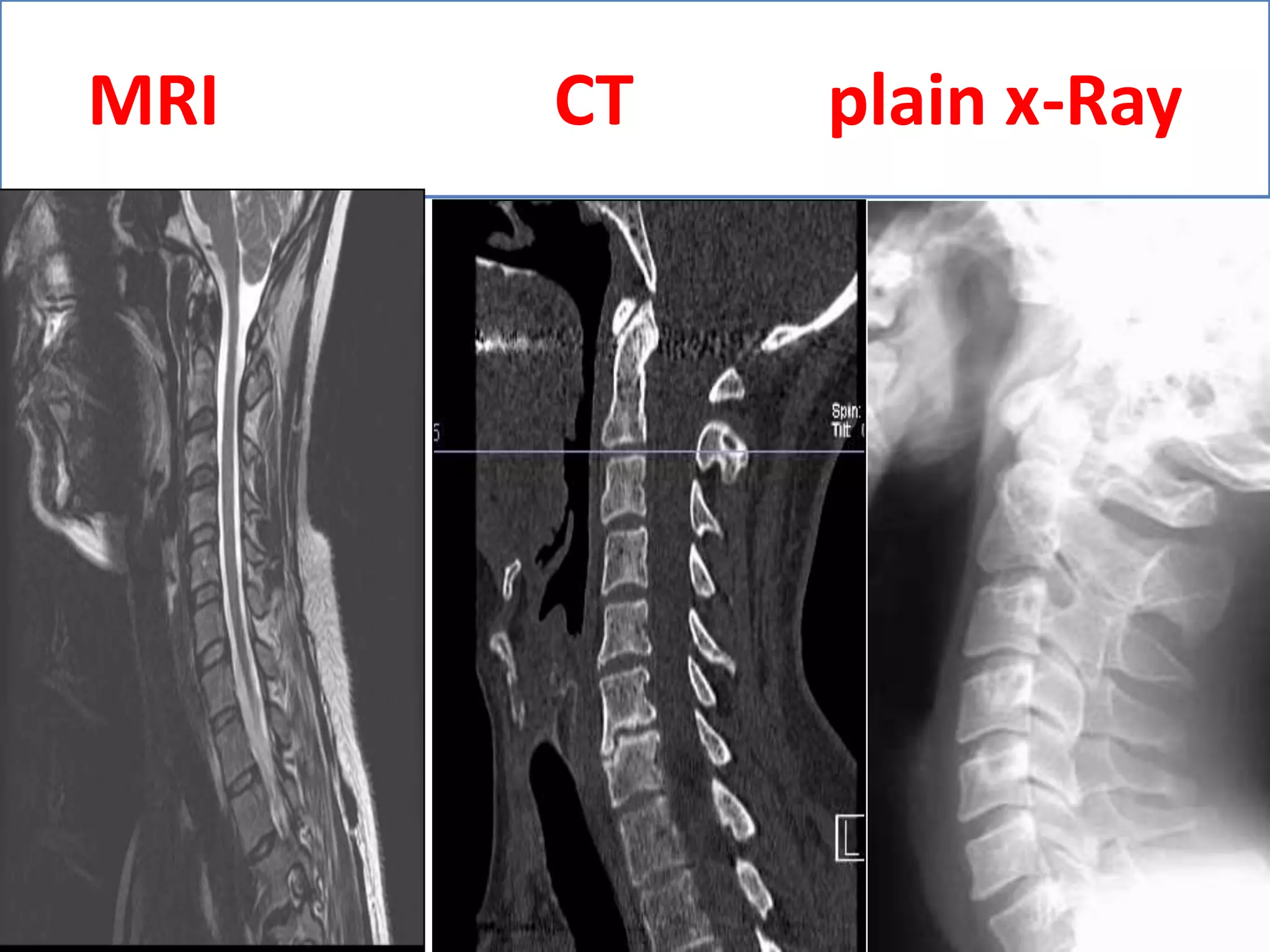
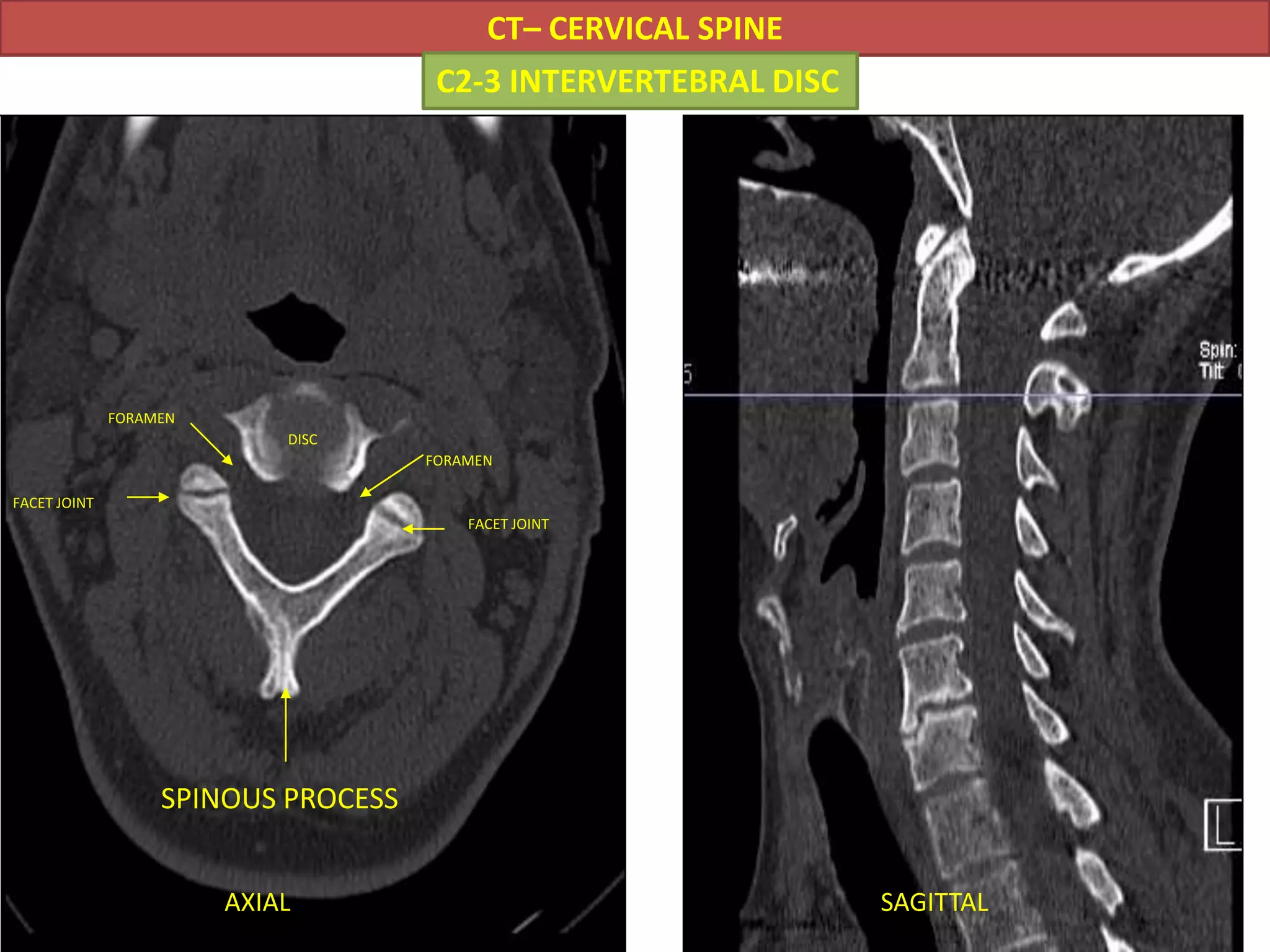
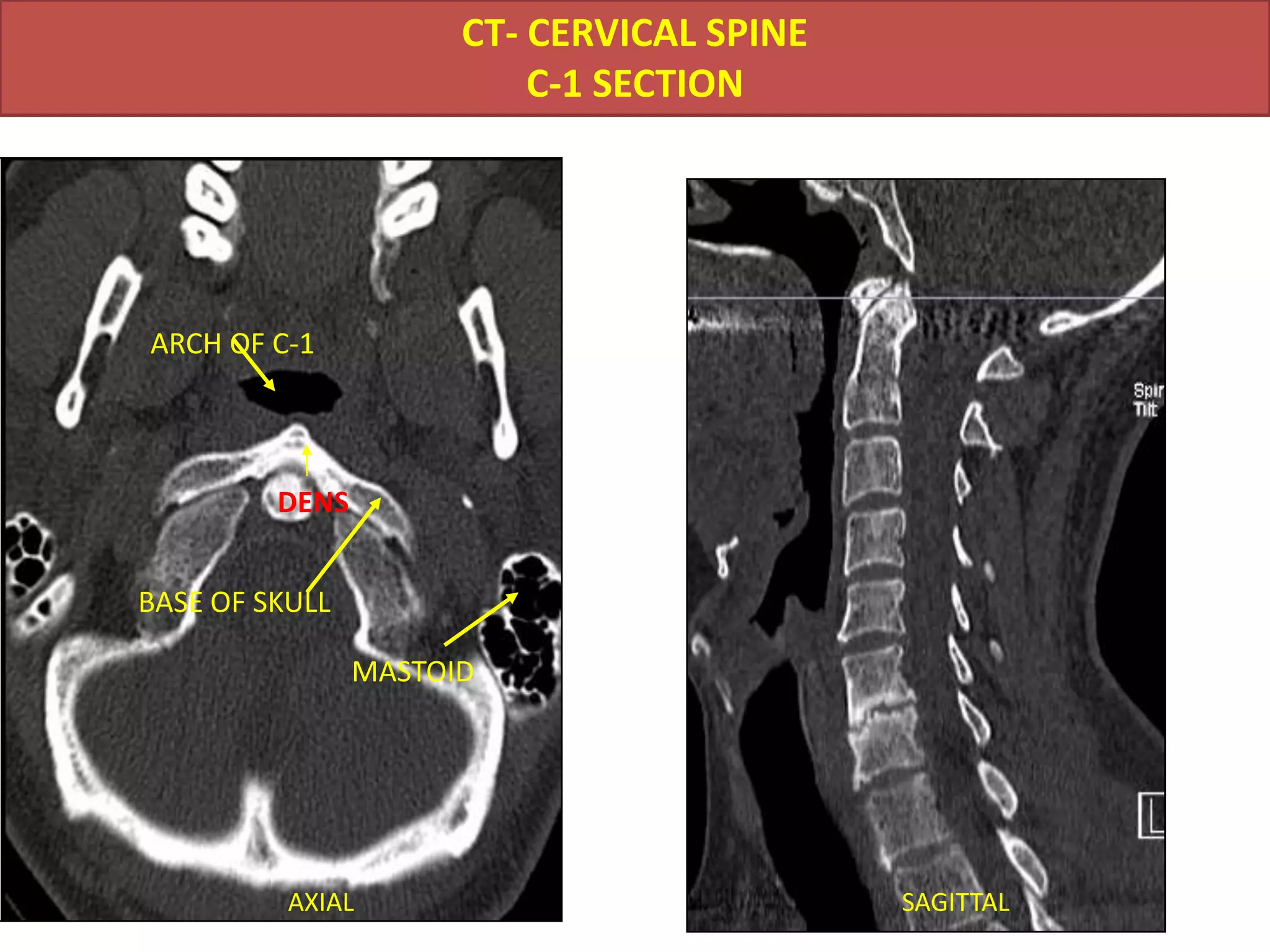
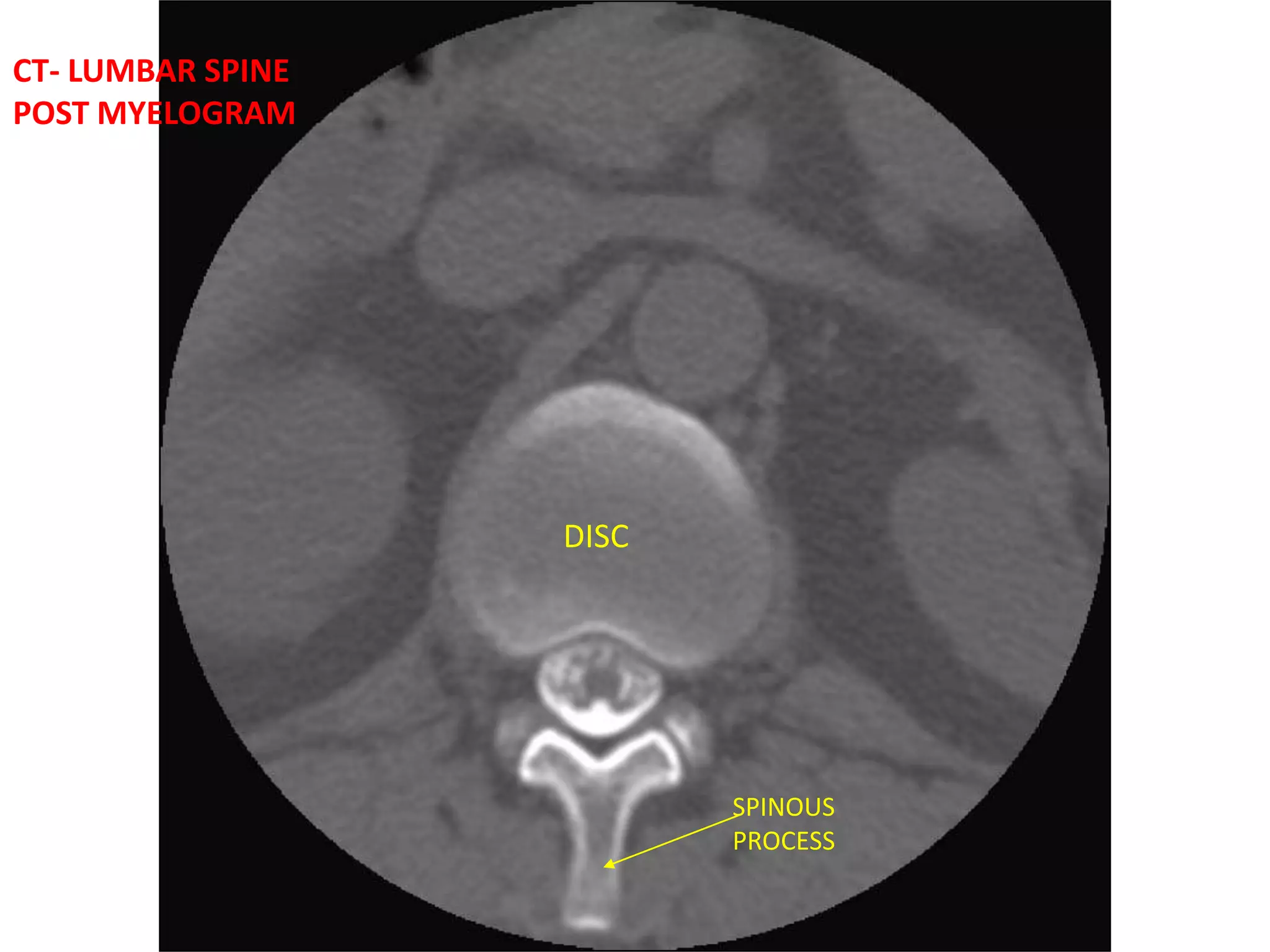
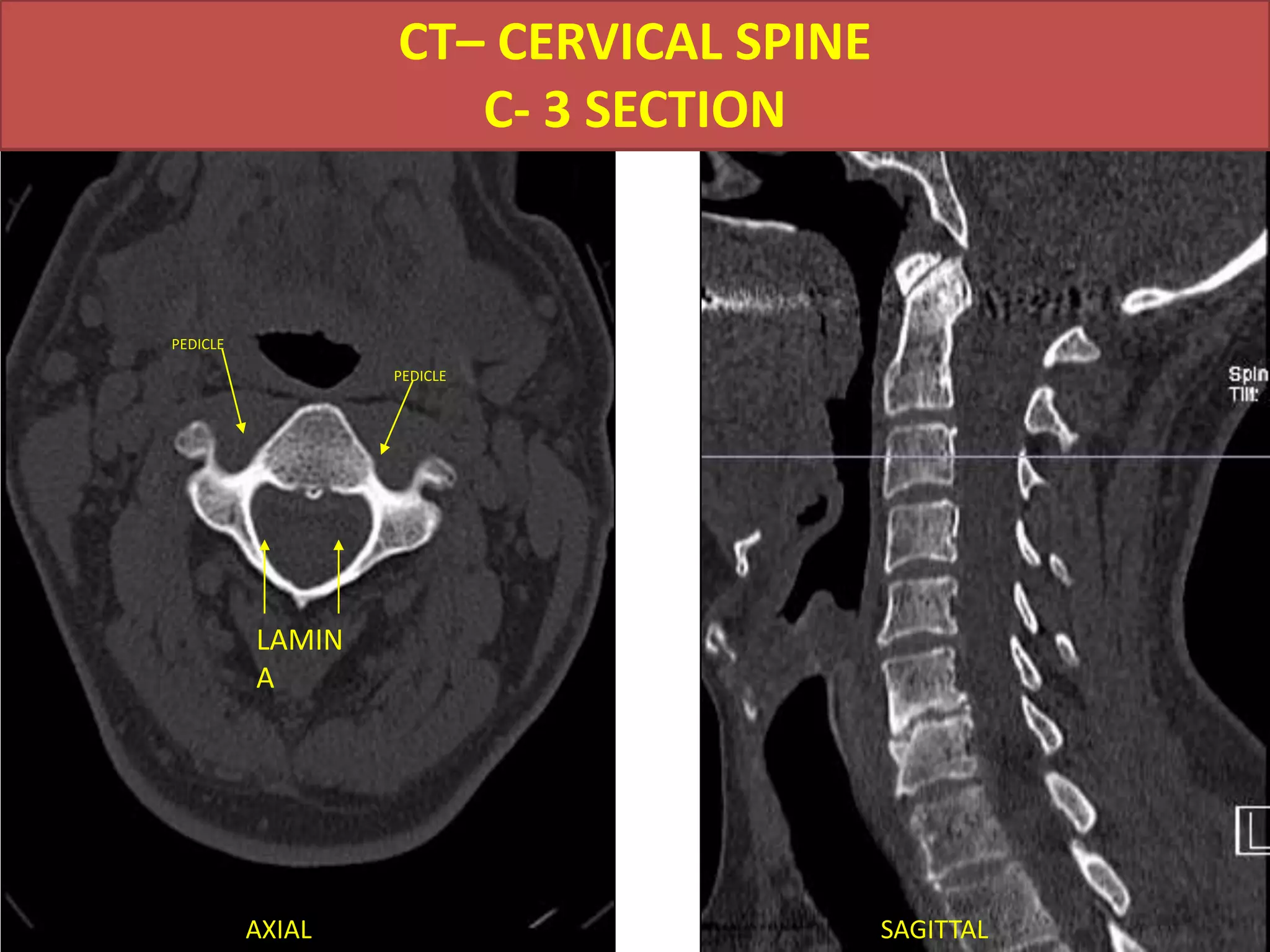
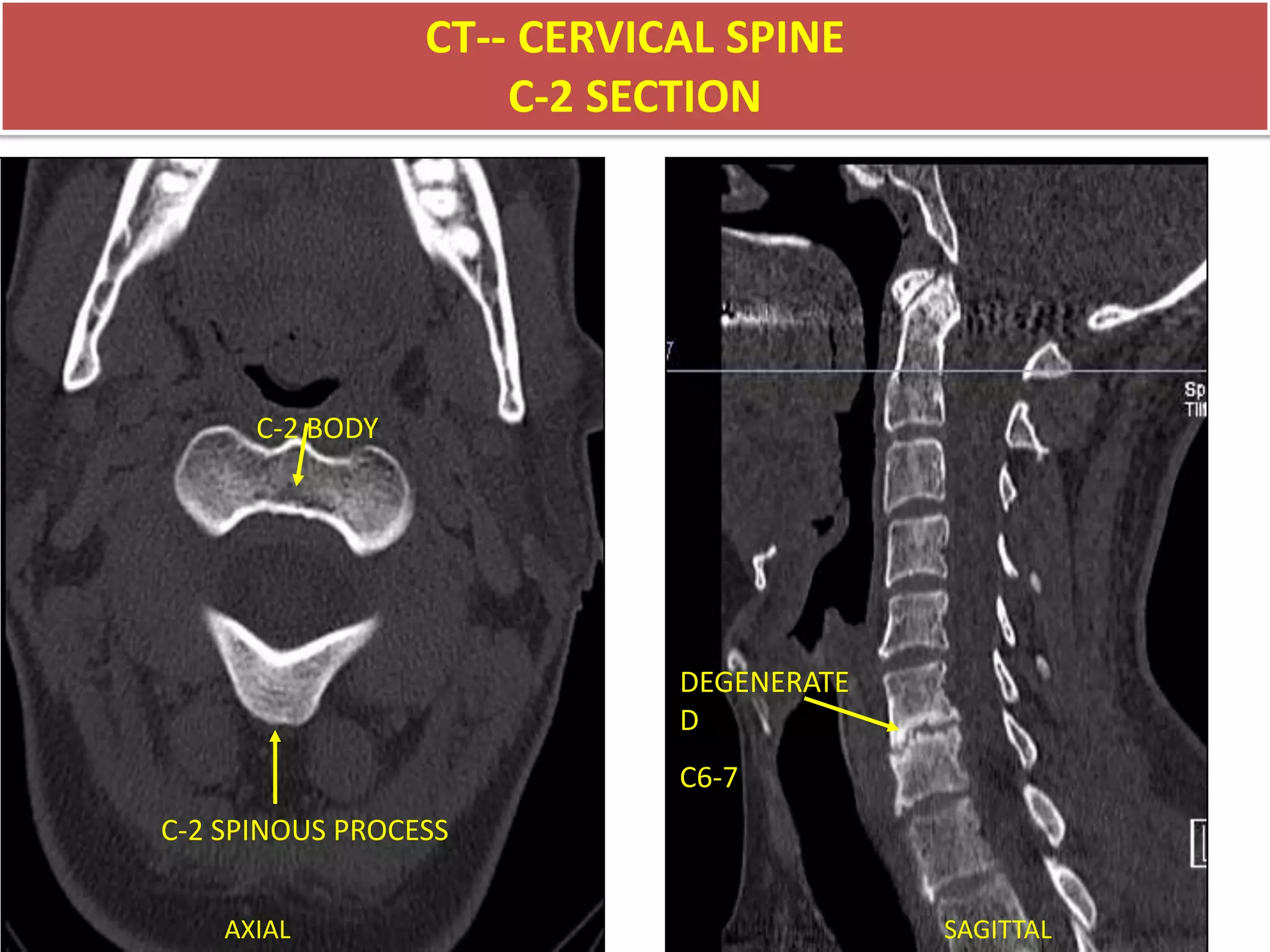
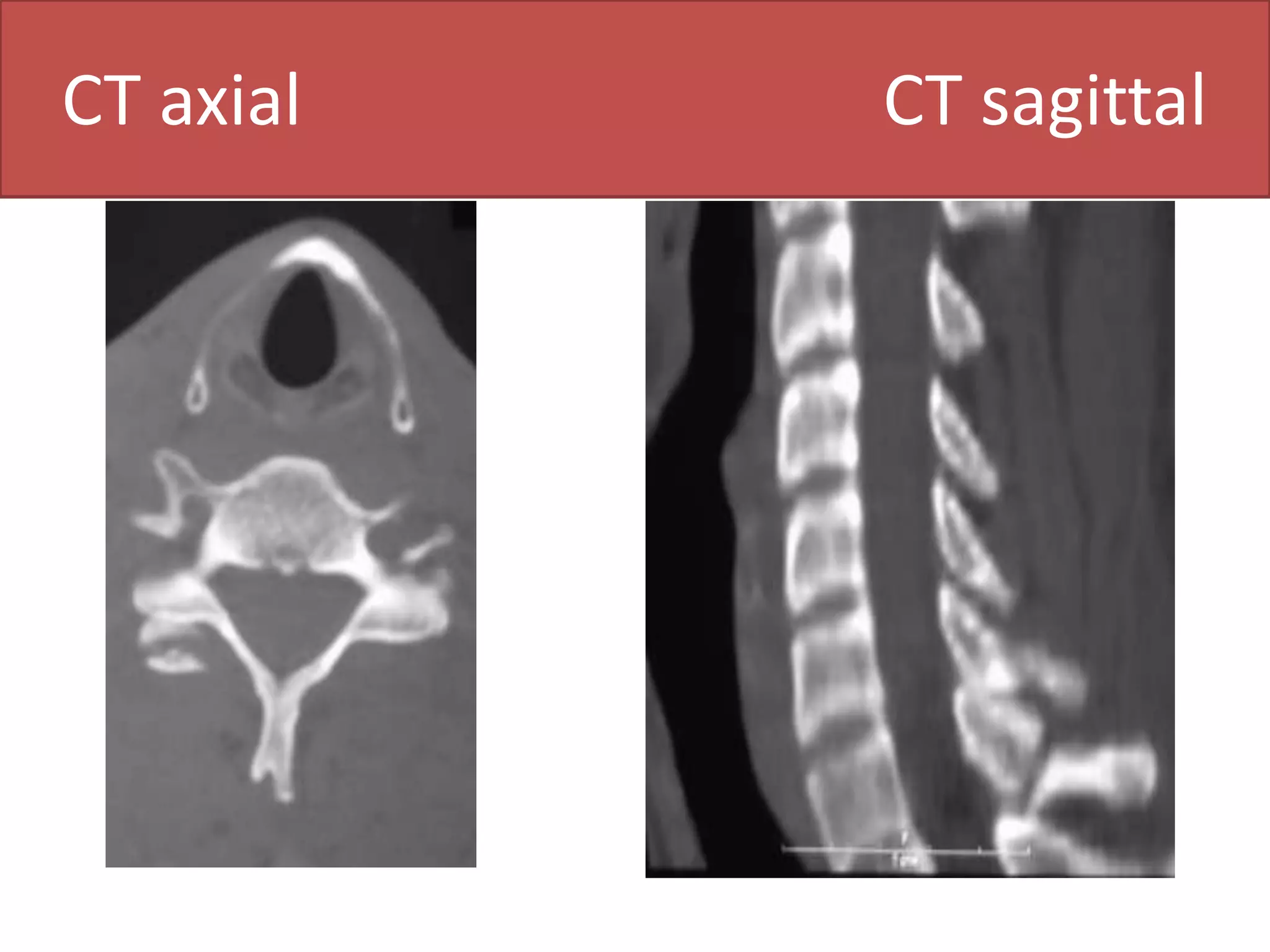
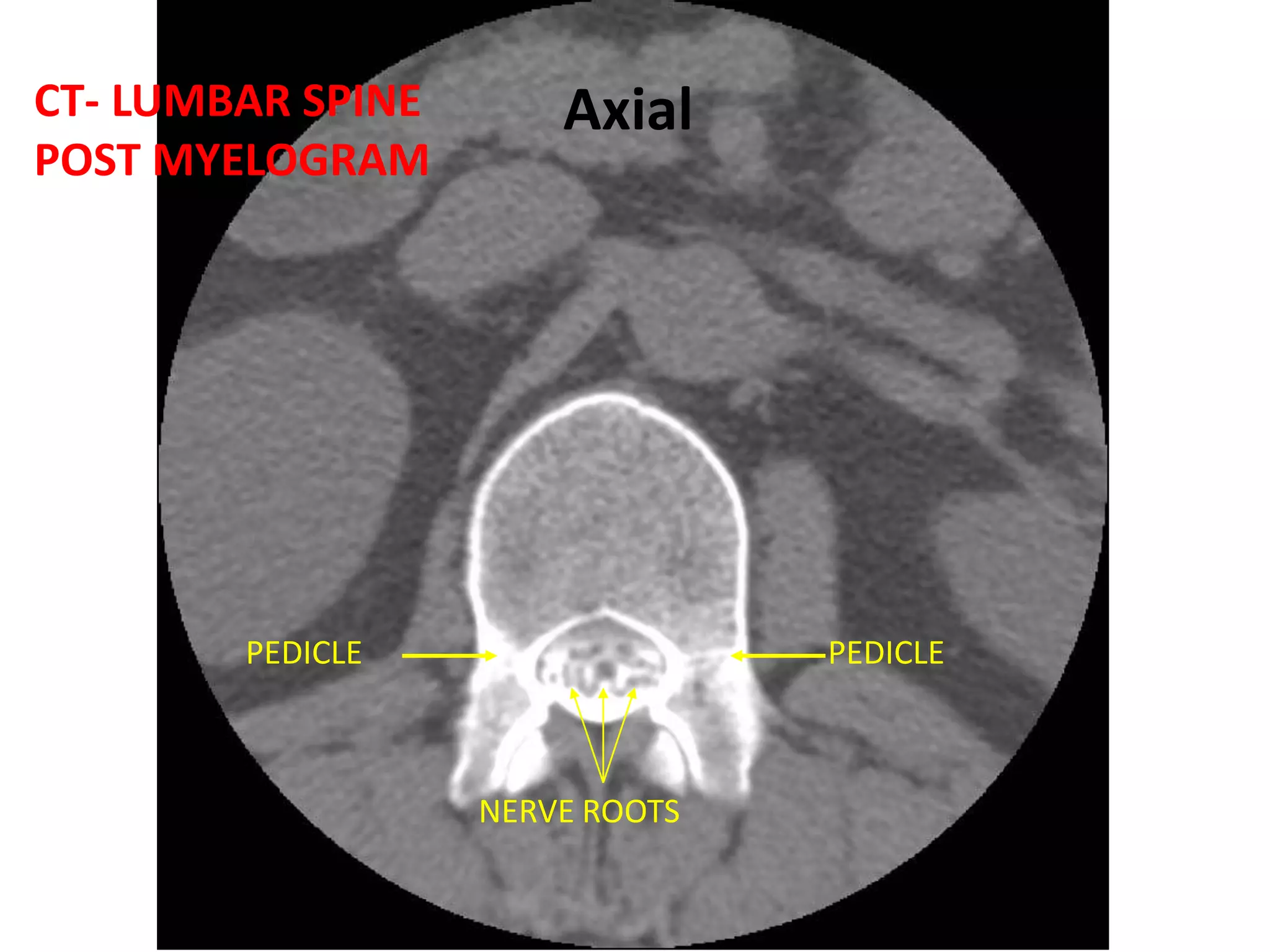
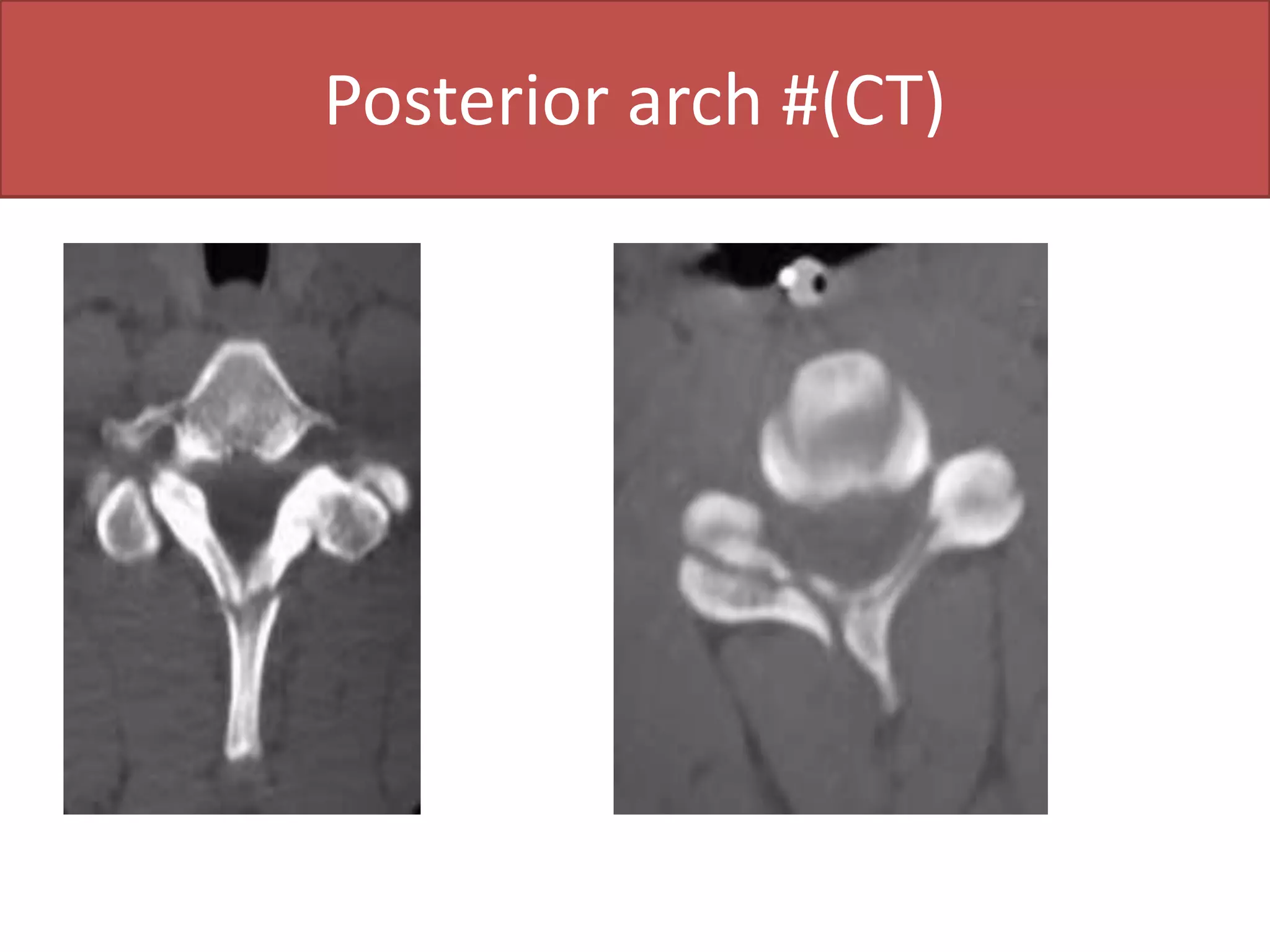
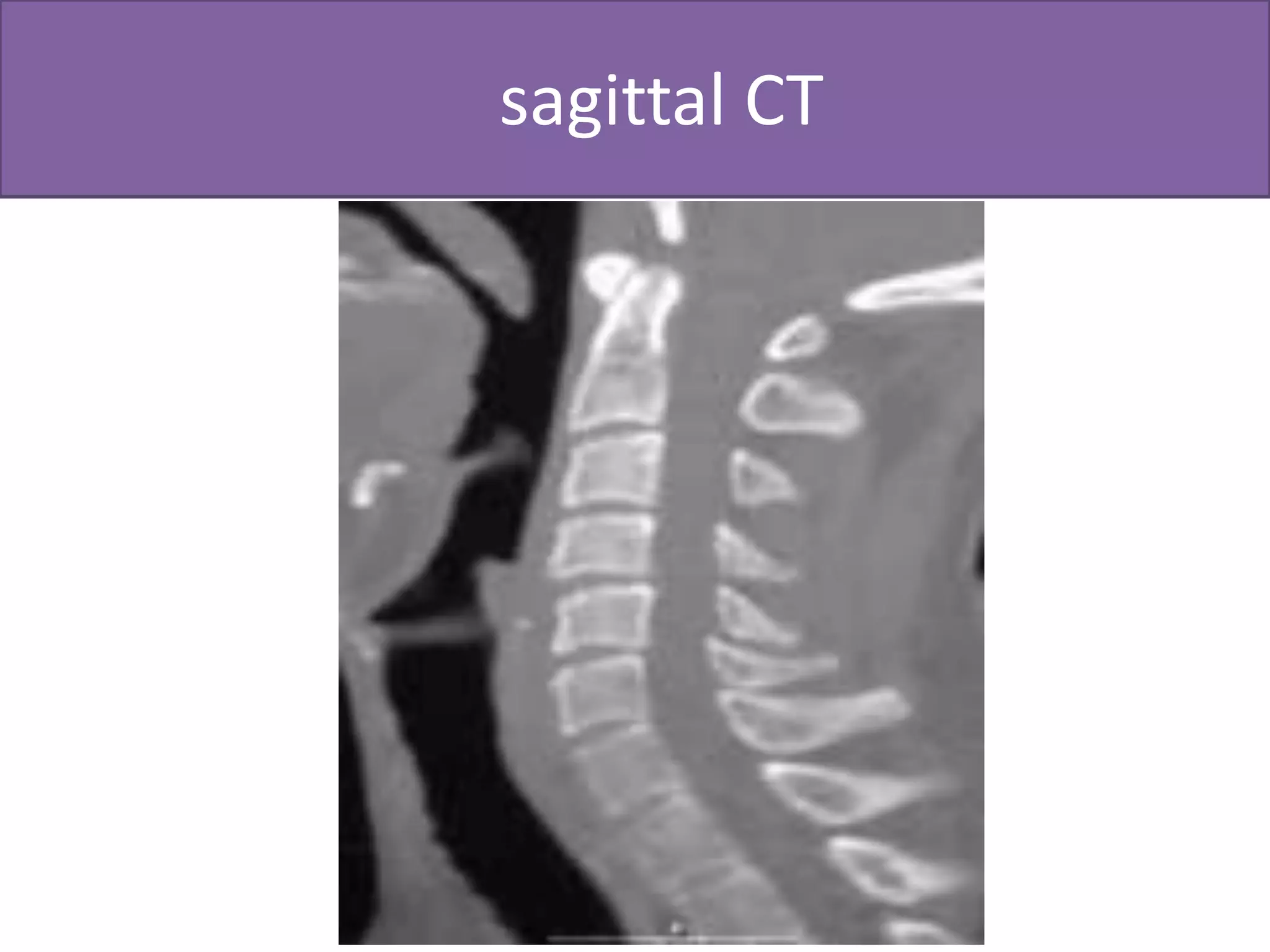
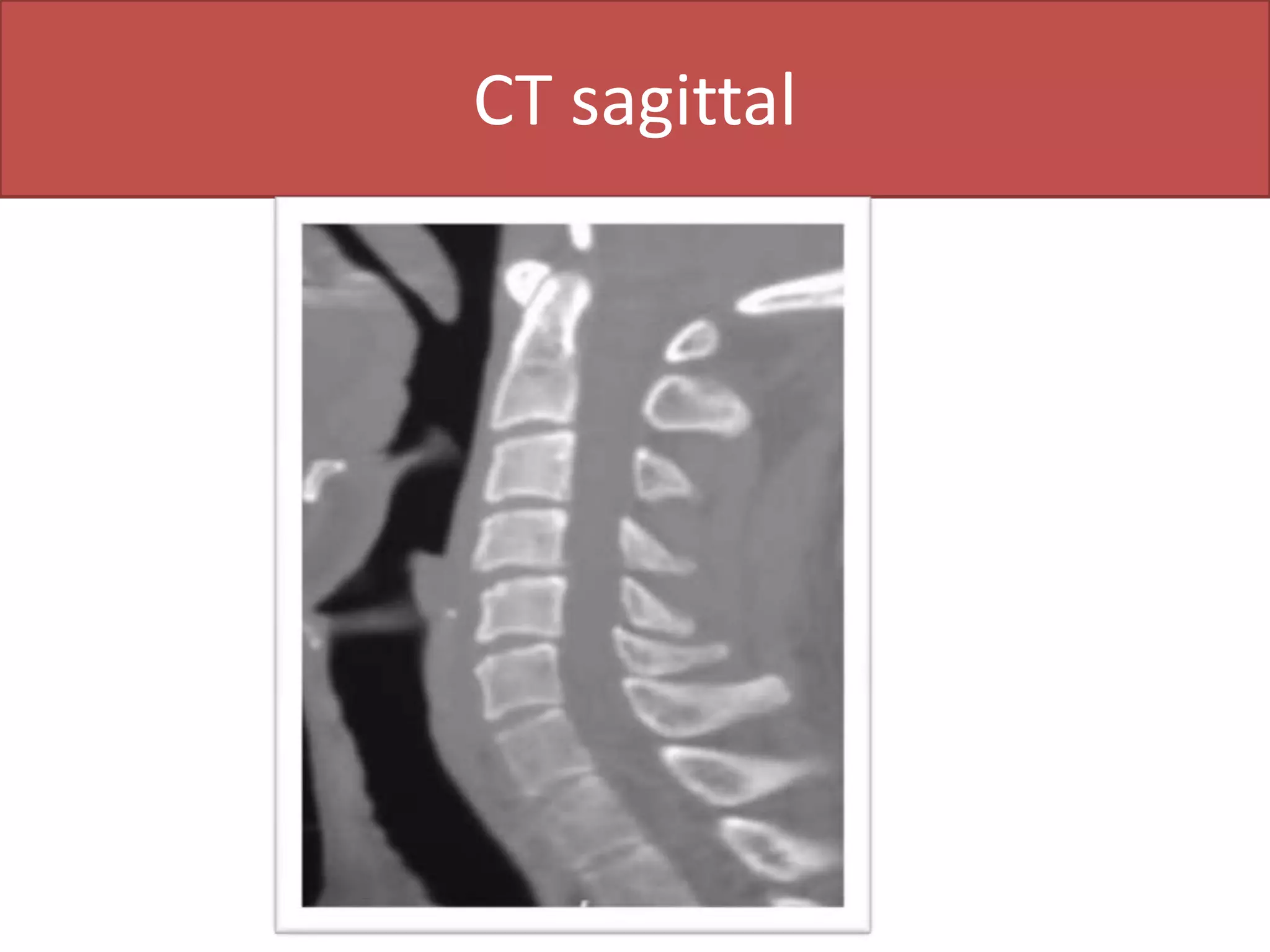
MRI and CT scans are commonly used to evaluate the spine for various indications such as disc lesions, postoperative evaluation, tumors, degenerative diseases, trauma, and congenital abnormalities. Preparations for CT and MRI may include fasting and administration of contrast material. Contrast is used for postoperative lumbar spine, inflammatory disorders, and neoplastic lesions but not for disc lesions or trauma. CT provides bone and soft tissue windows while MRI is better for visualizing soft tissues like discs and spinal cord. Both are useful for evaluating spinal structures.