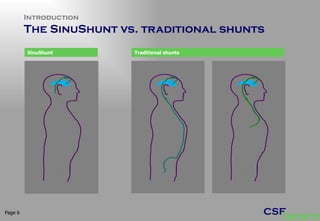
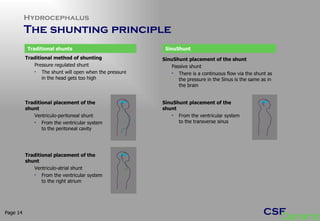
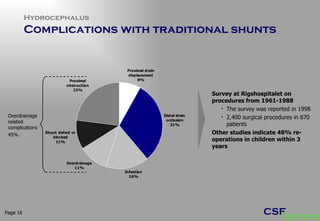
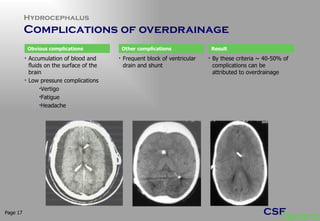
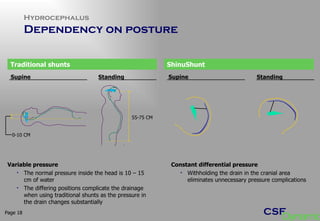
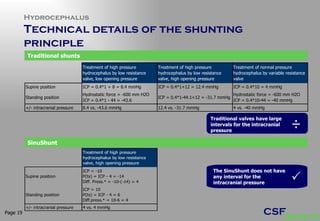
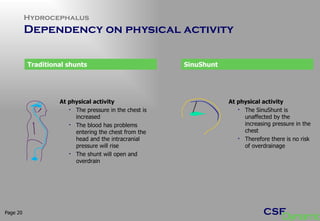
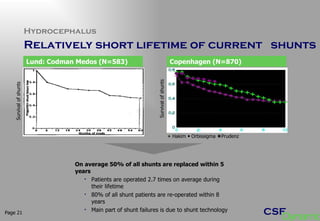
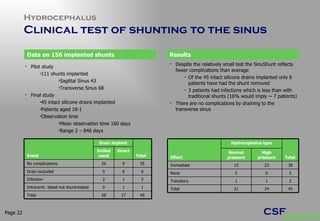
The document provides information on CSF Dynamics and their SinuShunt device for treating hydrocephalus. It discusses the shortcomings of traditional shunts, including numerous complications from overdrainage and short lifetimes. The SinuShunt aims to address these issues by draining cerebrospinal fluid from the brain ventricles directly into the transverse sinus, mimicking natural drainage and minimizing complications. Over 200 SinuShunts have been implanted with fewer reported complications compared to traditional shunts.