Downloaded 63 times



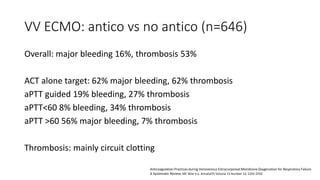
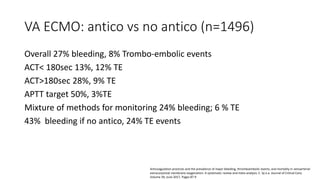
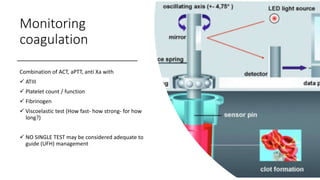

The document discusses anticoagulation management during veno-venous and venoarterial extracorporeal membrane oxygenation (ECMO), highlighting the balance between bleeding and thromboembolic events. It presents various anticoagulation strategies, including unfractionated heparin, low-molecular-weight heparin, and direct thrombin inhibitors, along with monitoring parameters like ACT, APTT, and anti-Xa levels. The review emphasizes the importance of tailored anticoagulation practices to minimize complications during ECMO therapy.



















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



