Downloaded 12 times
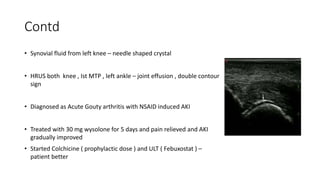
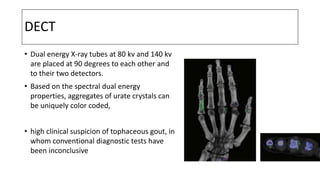
![US finding
• Hyperechoic deposition on the surface of
the articular hyaline cartilage, namely, a
double contour sign, suggested gout with a
sensitivity of 36.8% and a specificity of
97.3%
The characteristic US appearance of a tophus
includes an anechoic halo and hyperechoic
heterogeneous center [16] (Figure 5). The
peripheral anechoic halo likely represents the
fibrovascular zone](https://image.slidesharecdn.com/crystalsinrheumaticdiseases-221212194934-3027cf8a/85/Crystals-in-rheumatic-diseases-pptx-12-320.jpg)



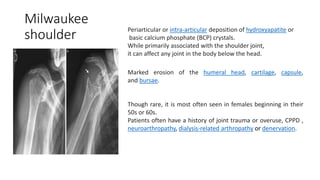

This document discusses various types of crystals found in rheumatology, including mono-sodium urate (gout), calcium pyrophosphate dehydrate (CPPD), basic calcium phosphate (BCP), cholesterol crystal, lipid crystal, and corticosteroid crystal. It presents several case studies demonstrating the clinical presentation and investigations for patients with these various crystal-related arthritides. Key points include the importance of identifying crystals in synovial fluid to confirm diagnoses, characteristic radiographic and ultrasound findings, and treatment approaches for acute flares and long-term management.





























































![reno protection [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/renoprotectionautosaved-231120105900-4e656917-thumbnail.jpg?width=640&height=640&fit=bounds)
























