Let’s start !
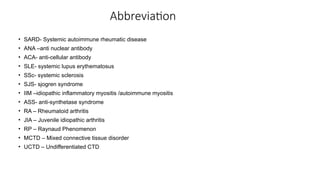
Antinuclearantibodies (ANA) refer to an autoantibody directed at material within the
nucleus of a cell.
It can target any part of nucleus
Even it can target Cytoplasm
Better term –anti-cellular antibody (ACA )
Seen in upto 30% healthy
Supportive for identifying autoimmune disease
4.
History at aglance !
Hargraves in 1948 discovered L.E. cell
Immunoflurescence technique helped to detect ANA
Initially used rat or mice cell substrate
Hep 2 cell – gold standard cell substrate for high
sensitivity
Latest – Hep 2000 with transfected Ro52
5.
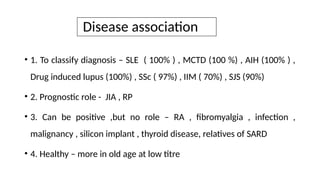
Disease association
• 1.To classify diagnosis – SLE ( 100% ) , MCTD (100 %) , AIH (100% ) ,
Drug induced lupus (100%) , SSc ( 97%) , IIM ( 70%) , SJS (90%)
• 2. Prognostic role - JIA , RP
• 3. Can be positive ,but no role – RA , fibromyalgia , infection ,
malignancy , silicon implant , thyroid disease, relatives of SARD
• 4. Healthy – more in old age at low titre
6.
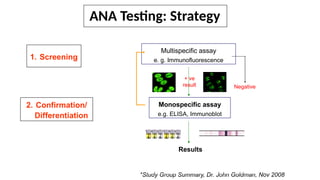
ANA Testing: Strategy
1.Screening
Multispecific assay
e. g. Immunofluorescence
+ ve
result
Monospecific assay
e.g. ELISA, Immunoblot
Results
2. Confirmation/
Differentiation
Negative
*Study Group Summary, Dr. John Goldman, Nov 2008
7.
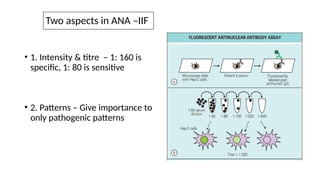
Two aspects inANA –IIF
• 1. Intensity & titre – 1: 160 is
specific, 1: 80 is sensitive
• 2. Patterns – Give importance to
only pathogenic patterns
ANA –IIF (nuclear pattern)
• AC 1- 14 & AC 29 – Nuclear Pattern
• Most common in SARD
• SLE , SSc, SJS , IIM , ASS , MCTD , UCTD and other SARD
12.
CASE 1
• 25year old female presented with fever , polyarthritis , malar area rash
and oral ulcer .
• Examination – BP- 170/100 , cervical lymph node +
• Basic investigation – CBC- 8/ 2700 /50 k , Urine R/M- Protein 2+ , RC-10,
PC -10 , Urine SPCR- 2.0 .
• Clinical Diagnosis ?
• Which is the method to be used here to detect ANA ?
- ANA –indirect immunofluorescence (IIF) by Hep 2
13.
Immunological report
• ANA–IIF ( Hep 2) – 4 (+) Homogenous at 1: 160 dilution
• dsDNA – positive ( by ELISA / Crithidia assay )
• C3 – 45 , C4 – 8
• Final Diagnosis ? Systemic lupus erythematosus with major flare
• ANA immunoblot ? Nucleosome 3+ , Rib P Protein 2+ , Sm 3+
14.
Case 2
• A40-year-old lady came to OPD with pain and swelling in both wrist , and MCP joints for
6 months
• She denied any extra-articular features
• Outside GP ordered RA factor, ANA – IIF.
• RA factor – 350 ( < 20 ) , ANA – 3+ Homogenous
• Diagnosis ? Seropositive RA
• Just ANA positivity alone is not sufficient to make it diagnosis of CTD
• What extra can be done ? 1. ANA blot ( if finance permits ) , 2 . Regular follow up ( more
important )
15.
Case 3
• A5 year old female child came with pain and swelling in both knees for 5 months
• Infection and malignancy screening ruled out
• Investigation – Raised ESR and CRP , RA factor negative , ANA – 3 + Homogenous
• Diagnosis ? ANA positive oligoarticular JIA
• What extra caution ? Regular eye screening for asymptomatic uveitis
16.
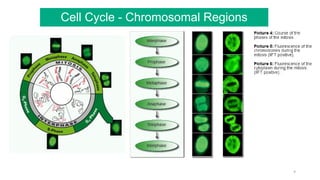
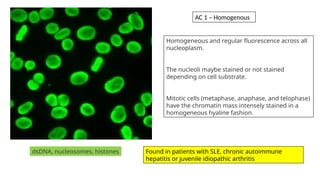
Homogeneous and regularfluorescence across all
nucleoplasm.
The nucleoli maybe stained or not stained
depending on cell substrate.
Mitotic cells (metaphase, anaphase, and telophase)
have the chromatin mass intensely stained in a
homogeneous hyaline fashion.
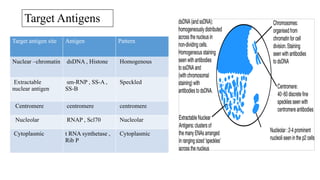
dsDNA, nucleosomes, histones Found in patients with SLE, chronic autoimmune
hepatitis or juvenile idiopathic arthritis
AC 1 – Homogenous
17.
Case 4
• A20-year-old college girl came to OPD with complaints of aches in her
body
• She has migraine headache , palpitation
• Examination – joints are hypermobile , Inv – ESR , CRP , RA factor
normal
• Outside GP did ANA – IIF and found 3 + nuclear dense fine speckled
• She started HCQ and was labelled as CTD
• What is your diagnosis?
18.
Diagnosis ?
• Thisis a case of fibromyalgia
• There is no clinical evidence of CTD
• ANA – nuclear DFS is normal and it rules out SARD
• Stop HCQ
• Assure the patient that she does not have any autoimmune problem.
• Learning point?
• ANA is supportive of clinical diagnosis; it has no stand-alone role to make a diagnosis
19.
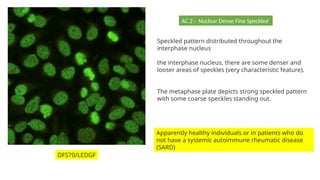
Speckled pattern distributedthroughout the
interphase nucleus
the interphase nucleus, there are some denser and
looser areas of speckles (very characteristic feature).
The metaphase plate depicts strong speckled pattern
with some coarse speckles standing out.
Apparently healthy individuals or in patients who do
not have a systemic autoimmune rheumatic disease
(SARD)
DFS70/LEDGF
AC 2 - Nuclear Dense Fine Speckled
20.
Case 4
• 40year old lady with bluish discoloration of tip of fingers , reflux symptoms and
thickening of skin of the fingers came to OPD
• Examination – active RP , skin thickening upto elbow , facial telangiectasia
• Investigation – Esophageal dismotility in Ba swallow
• Clinical Diagnosis ?Limited scleroderma
• ANA –IIF ? 4 + centromere at 1:160 dilution
• Do you need any ANA blot ? Ideally no
21.
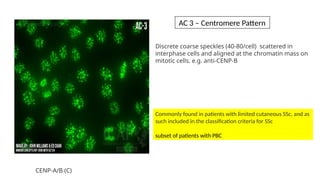
Discrete coarse speckles(40-80/cell) scattered in
interphase cells and aligned at the chromatin mass on
mitotic cells. e.g. anti-CENP-B
Commonly found in patients with limited cutaneous SSc, and as
such included in the classification criteria for SSc
subset of patients with PBC
CENP-A/B (C)
AC 3 – Centromere Pattern
22.
Case 5
• A30 year old lady presented in emergency with weakness in four limbs
, found to have hypokalemia , similar episode in past
• She gave history of mild dryness of mouth, eyes and dental caries
• Investigation – K – 2.3 , HC03- 12 , C3 – 45 , C4- 12
• Clinical diagnosis ? Hypokalemic periodic palsy in a case of Sjogren
syndrome
• ANA-IIF ( Hep 2000 ) – 4 + fine speckled pattern
• Any other test ? Anti SS A (R060) and SS B (La) (Immunoassay /ELISA ) –
need for classification criteria .
23.
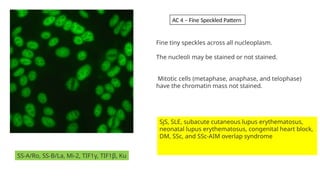
SS-A/Ro, SS-B/La, Mi-2,TIF1γ, TIF1β, Ku
Fine tiny speckles across all nucleoplasm.
The nucleoli may be stained or not stained.
Mitotic cells (metaphase, anaphase, and telophase)
have the chromatin mass not stained.
SjS, SLE, subacute cutaneous lupus erythematosus,
neonatal lupus erythematosus, congenital heart block,
DM, SSc, and SSc-AIM overlap syndrome
AC 4 – Fine Speckled Pattern
24.
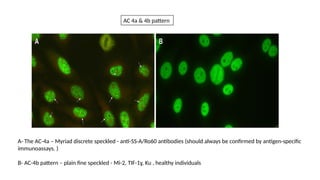
A- The AC-4a– Myriad discrete speckled - anti-SS-A/Ro60 antibodies (should always be confirmed by antigen-specific
immunoassays. )
B- AC-4b pattern – plain fine speckled - Mi-2, TIF-1ɣ, Ku , healthy individuals
AC 4a & 4b pattern
25.
Anti-SS-A/Ro (Ro60) andAIM-specific autoantibodies may
be undetected in HEp-2 IIFA-screening
The HEp-2000 cell line is a modified substrate of the HEp-2 cell line that
has been genetically engineered to increase the expression of SS-A/Ro60
in transfected cells
26.
Case 6
• 30year old lady came with puffiness of fingers , arthritis ,
discoloration of finger tips
• Examination – active RP , puffy fingers
• Inv – HRCT chest showed ILD
• Clinical diagnosis ?
• Mixed connective tissue disorder (MCTD)
• ANA –IIF – 4 + coarse speckled ( part of classification criteria of
MCTD )
• What other immunological test – U1 RNP test ( blot / ELISA )
27.
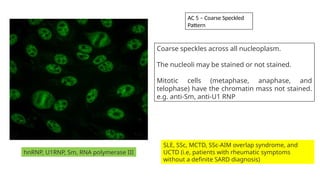
hnRNP, U1RNP, Sm,RNA polymerase III
SLE, SSc, MCTD, SSc-AIM overlap syndrome, and
UCTD (i.e, patients with rheumatic symptoms
without a definite SARD diagnosis)
Coarse speckles across all nucleoplasm.
The nucleoli may be stained or not stained.
Mitotic cells (metaphase, anaphase, and
telophase) have the chromatin mass not stained.
e.g. anti-Sm, anti-U1 RNP
AC 5 – Coarse Speckled
Pattern
28.
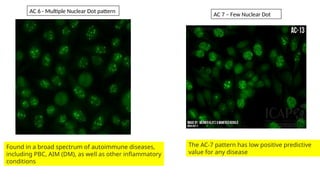
Found in abroad spectrum of autoimmune diseases,
including PBC, AIM (DM), as well as other inflammatory
conditions
AC 6 - Multiple Nuclear Dot pattern
AC 7 – Few Nuclear Dot
The AC-7 pattern has low positive predictive
value for any disease
29.
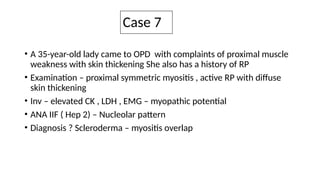
Case 7
• A35-year-old lady came to OPD with complaints of proximal muscle
weakness with skin thickening She also has a history of RP
• Examination – proximal symmetric myositis , active RP with diffuse
skin thickening
• Inv – elevated CK , LDH , EMG – myopathic potential
• ANA IIF ( Hep 2) – Nucleolar pattern
• Diagnosis ? Scleroderma – myositis overlap
30.
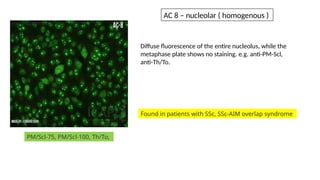
Diffuse fluorescence ofthe entire nucleolus, while the
metaphase plate shows no staining. e.g. anti-PM-Scl,
anti-Th/To.
PM/Scl-75, PM/Scl-100, Th/To,
Found in patients with SSc, SSc-AIM overlap syndrome
AC 8 – nucleolar ( homogenous )
31.
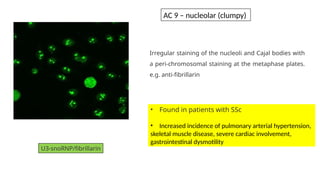
Irregular staining ofthe nucleoli and Cajal bodies with
a peri-chromosomal staining at the metaphase plates.
e.g. anti-fibrillarin
U3-snoRNP/fibrillarin
• Found in patients with SSc
• Increased incidence of pulmonary arterial hypertension,
skeletal muscle disease, severe cardiac involvement,
gastrointestinal dysmotility
AC 9 – nucleolar (clumpy)
32.
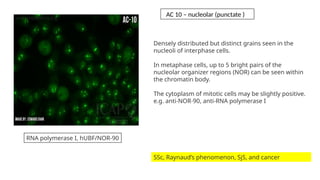
Densely distributed butdistinct grains seen in the
nucleoli of interphase cells.
In metaphase cells, up to 5 bright pairs of the
nucleolar organizer regions (NOR) can be seen within
the chromatin body.
The cytoplasm of mitotic cells may be slightly positive.
e.g. anti-NOR-90, anti-RNA polymerase I
SSc, Raynaud’s phenomenon, SjS, and cancer
RNA polymerase I, hUBF/NOR-90
AC 10 – nucleolar (punctate )
33.
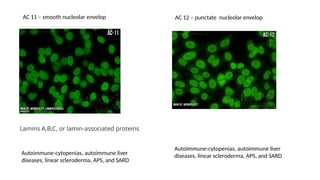
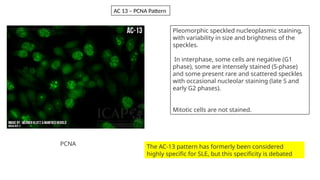
Autoimmune-cytopenias, autoimmune liver
diseases,linear scleroderma, APS, and SARD
Lamins A,B,C, or lamin-associated proteins
AC 11 – smooth nucleolar envelop AC 12 – punctate nucleolar envelop
Autoimmune-cytopenias, autoimmune liver
diseases, linear scleroderma, APS, and SARD
34.
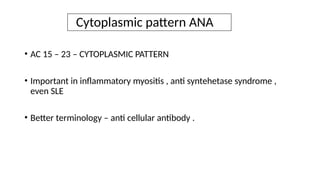
Pleomorphic speckled nucleoplasmicstaining,
with variability in size and brightness of the
speckles.
In interphase, some cells are negative (G1
phase), some are intensely stained (S-phase)
and some present rare and scattered speckles
with occasional nucleolar staining (late S and
early G2 phases).
Mitotic cells are not stained.
The AC-13 pattern has formerly been considered
highly specific for SLE, but this specificity is debated
AC 13 – PCNA Pattern
PCNA
35.
Cytoplasmic pattern ANA
•AC 15 – 23 – CYTOPLASMIC PATTERN
• Important in inflammatory myositis , anti syntehetase syndrome ,
even SLE
• Better terminology – anti cellular antibody .
36.
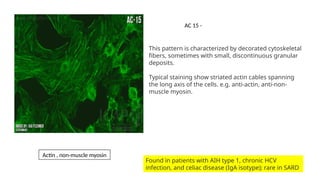
This pattern ischaracterized by decorated cytoskeletal
fibers, sometimes with small, discontinuous granular
deposits.
Typical staining show striated actin cables spanning
the long axis of the cells. e.g. anti-actin, anti-non-
muscle myosin.
Found in patients with AIH type 1, chronic HCV
infection, and celiac disease (IgA isotype); rare in SARD
Actin , non-muscle myosin
AC 15 -
Case 8
• A40-year-old female with complaints of polyarthritis, breathlessness and new-onset
skin rash came to OPD
• Exam – Active RP, proximal myositis , Mechanic hand
• Inv- CK 250, LDH 450 , nail fold capillary changes
• Clinical Diagnosis? Anti synthetase syndrome
• ANA-IIF ( Hep 2) – 3 + Cytoplasmic Dense Fine Speckled
• Myositis Profile – PL 7 strong positive
39.
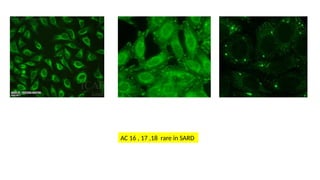
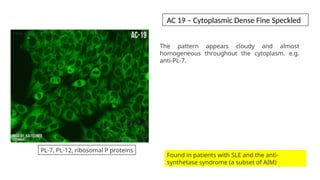
The pattern appearscloudy and almost
homogeneous throughout the cytoplasm. e.g.
anti-PL-7.
Found in patients with SLE and the anti-
synthetase syndrome (a subset of AIM)
PL-7, PL-12, ribosomal P proteins
AC 19 – Cytoplasmic Dense Fine Speckled
40.
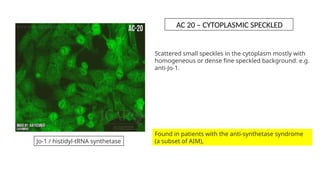
Scattered small specklesin the cytoplasm mostly with
homogeneous or dense fine speckled background. e.g.
anti-Jo-1.
Jo-1 / histidyl-tRNA synthetase
Found in patients with the anti-synthetase syndrome
(a subset of AIM),
AC 20 – CYTOPLASMIC SPECKLED
41.
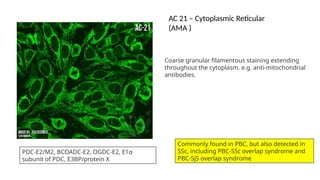
Coarse granular filamentousstaining extending
throughout the cytoplasm. e.g. anti-mitochondrial
antibodies.
PDC-E2/M2, BCOADC-E2, OGDC-E2, E1α
subunit of PDC, E3BP/protein X
Commonly found in PBC, but also detected in
SSc, including PBC-SSc overlap syndrome and
PBC-SjS overlap syndrome
AC 21 – Cytoplasmic Reticular
(AMA )
42.
Other cytoplasmic pattern
•AC 22 (Polar & Golgi Like ) – No definite association with SARD
• AC 23 (Rod & Ring) – IFN /Ribavirin therapy
43.
ANA – mitoticpattern
• Less seen in SARD
• AC 24 – 28 – clinical relevance is less
44.
Take home
• Mostsensitive screening is indirect immunofluorescent ANA assay
• Human Hep-2 cell can detect ANA in more than 95% of patients
• ANA-Hep2 can be negative if Ro Ab is there, hence HEP2000 newly used
• ANA -IIF is less specific while ANA-ELISA and Blot more specific test
• A positive ANA-IF test can be seen in autoimmune thyroid disease, drug-induced
lupus, infections, and neoplastic diseases.
• Some healthy individuals also have a positive IF results










































![reno protection [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/renoprotectionautosaved-231120105900-4e656917-thumbnail.jpg?width=640&height=640&fit=bounds)
























