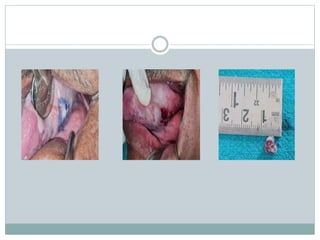
This document presents a case study of a 64-year-old male farmer diagnosed with verrucous leukoplakia. It summarizes the patient's medical history, including a long-term tobacco chewing habit. The clinical examination revealed grayish-white patches on the tongue and inner cheek. A biopsy was performed and histopathological examination confirmed the diagnosis of leukoplakia. The patient's long-term tobacco use likely caused the potentially malignant disorder, and he was prescribed medication and advised to quit chewing tobacco to prevent progression to oral cancer.

![ Ghazali et al., established the following criteria:
The lesion starts as homogenous leukoplakia without evidence of
dysplasia at the first visit
With time, some areas of leukoplakia become verrucous
The disease progresses to the development of multiple isolated or
confluent lesions at the same or a different site
With time, the disease progresses through the different
histopathological stages reported by Hansen et al.[2]
The appearance of new lesions after treatment
A follow-up period of no less than 1 year.
Gandolfo et al., establish the following criteria:
An initially innocuous lesion characterized by a homogenous plaque
that progresses over time to an exophytic, diffuse, usually multifocal,
lesion with a verrucous epithelial growth pattern
Histopathologically, proliferative verrucous leukoplakia (PVL)
changes gradually from a simple plaque of hyperkeratosis without
dysplasia to verrucous hyperplasia, verrucous carcinoma or oral
squamous cell carcinoma (OSCC).](https://image.slidesharecdn.com/verrucousleukoplakia-230607060827-a46507c9/85/Verrucous-leukoplakia-pptx-28-320.jpg)


























































![anurag14[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/anurag141-221219160230-80032896-thumbnail.jpg?width=640&height=640&fit=bounds)




























