Downloaded 23 times

![KRANIOPHARYNGEOM
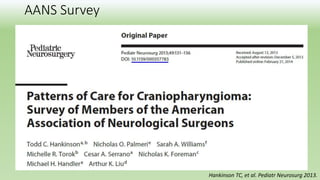
Grade of initial hypothalamic involvement was similar
2000 n=120
2001–2007
2007 n=106
2007–2012
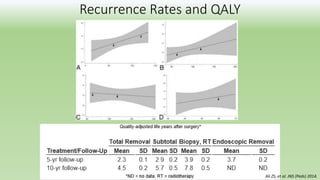
Radical 38% 18% [p=0.01]
Hypothalamus-sparing operations
resulting in no (further)
hypothalamic lesions
35% 13% [p=0.005]
Event-free-survival rates were similar in both cohorts
A trend towards less radical surgical approaches is observed
A reduced rate of severe hypothalamic lesions
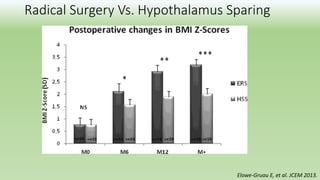
Radical surgery is not an appropriate treatment strategy in patients with hypothalamic involvement
Hoffman A, et al. 2014. Klinische Pädiatrie.](https://image.slidesharecdn.com/craniopharyngiomaconservativemanagement-180206054613/85/Craniopharyngioma-conservative-management-10-320.jpg)

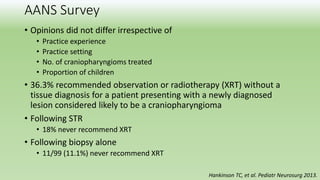
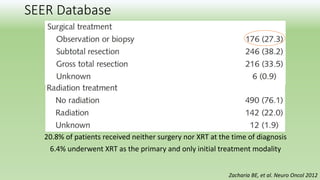
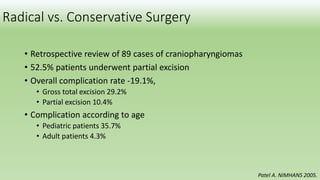
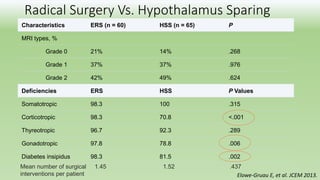
This document discusses different approaches to treating craniopharyngiomas, which are brain tumors that evoke strong emotions. It summarizes various studies that have looked at conservative treatment versus surgery, as well as radical surgery versus hypothalamus-sparing surgery. The findings are mixed, with some studies finding similar outcomes between radical and conservative approaches, while others found higher complication rates with radical surgery. Overall, the document suggests balancing different treatment approaches rather than being dogmatic, as craniopharyngiomas are complex tumors with variability in how they present and respond to treatment.

























































![Paroxysmal Sympathetic Hyperactivity in Traumatic Brain Injury [PSH in TBI]](https://cdn.slidesharecdn.com/ss_thumbnails/pshintbi-170825135752-thumbnail.jpg?width=640&height=640&fit=bounds)























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

