
Downloaded 34 times

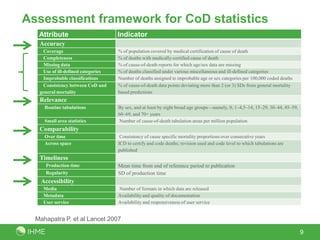
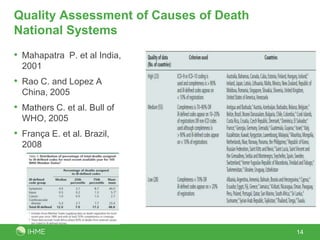
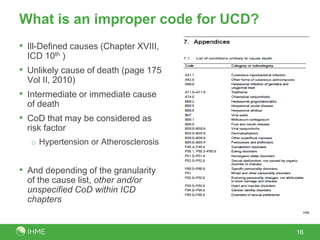
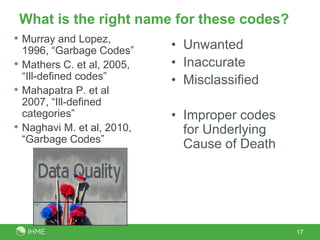
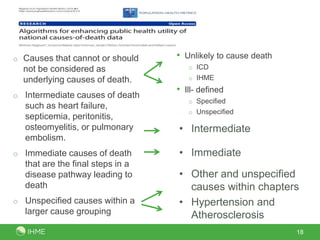
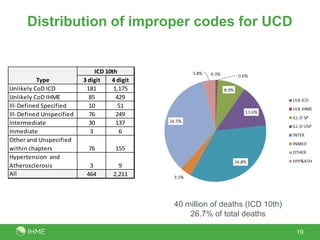
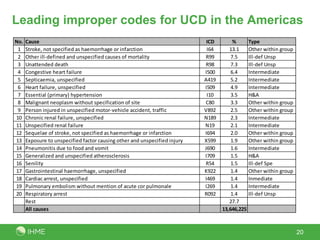
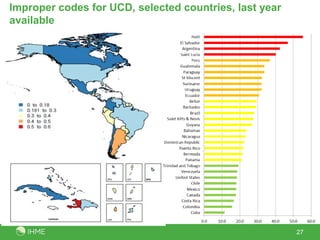
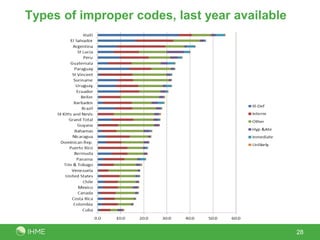
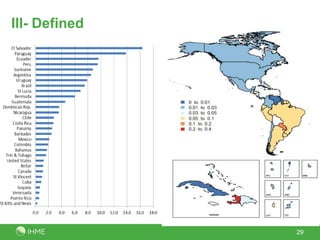
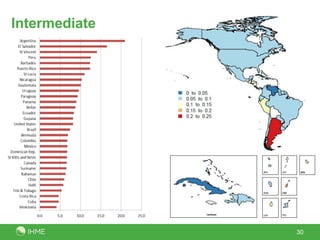
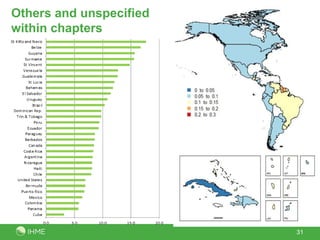
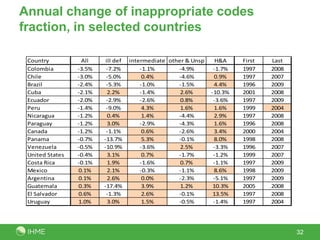
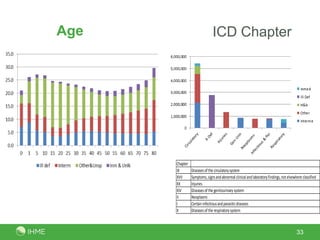

The document assesses the quality of mortality information and causes of death, focusing on definitions and frameworks for evaluating data quality. It outlines attributes for measuring data quality under the ICD framework, identifies improper coding for underlying causes of death, and highlights the prevalence of improper codes in various countries. The findings reveal that about 25% of deaths in the region are attributed to improper codes, indicating significant issues in mortality reporting.









































































































