Downloaded 66 times

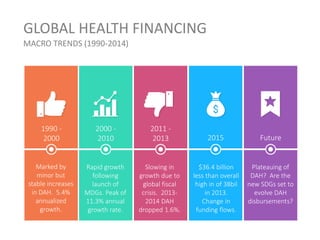







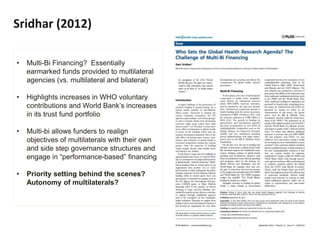
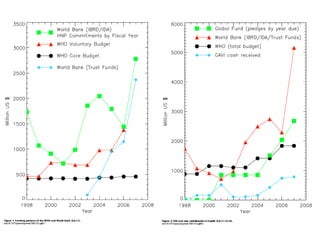
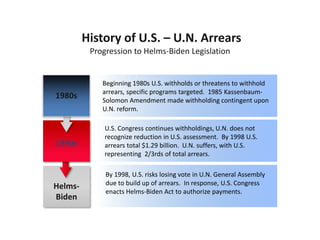
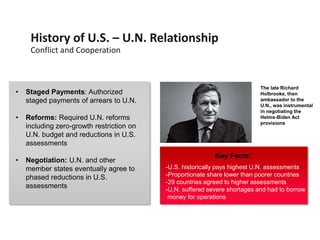
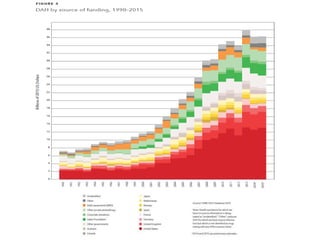
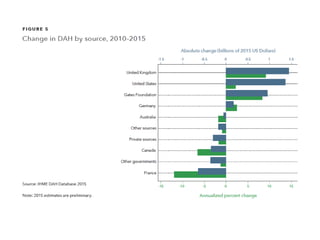
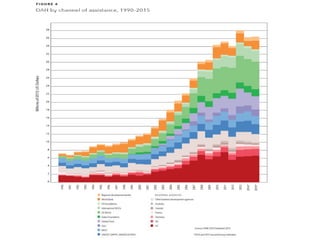


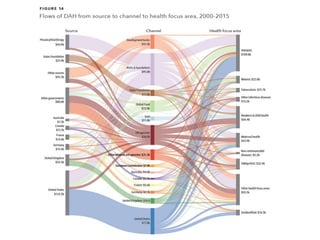

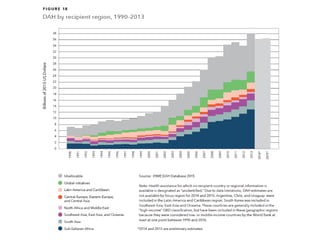
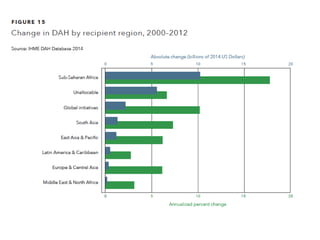
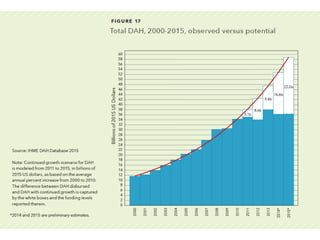
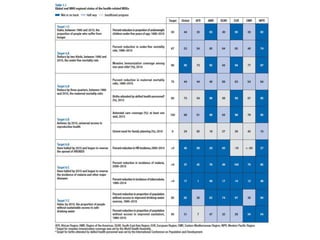


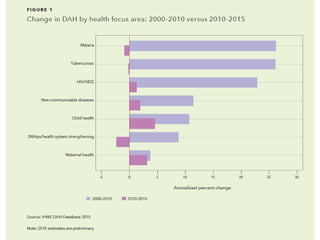


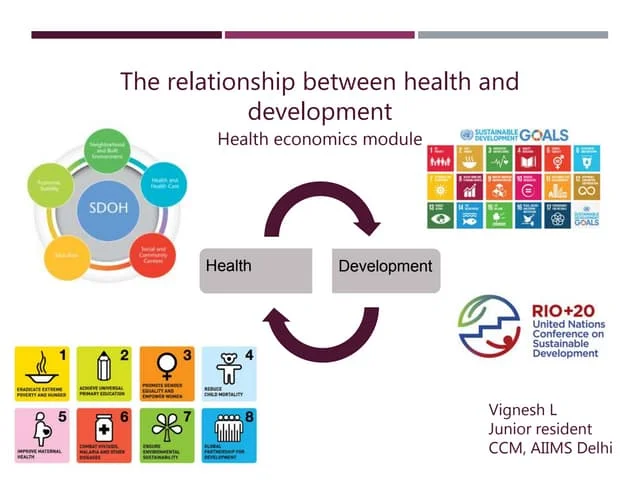
The document discusses global health financing, emphasizing the complexities and changes in donor assistance funding, with the U.S. being the largest contributor. It highlights trends in development assistance for health from 1990 to 2014, noting a period of growth followed by a decline, and the impact of various funding mechanisms on global health governance. Additionally, it covers historical U.S. involvement with the UN and the implications of financial policies on global health initiatives.