
Download as PDF, PPTX

![Eval questions to be explored qualitatively-1
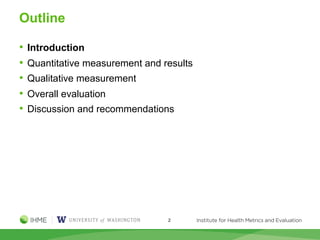
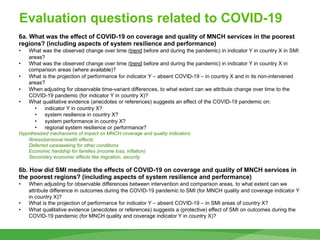
4. What was the contribution of SMI in the performance of health systems in the
region [note this question has overlap with question (3)]? What are the prospects for
sustainability of SMI interventions and results?
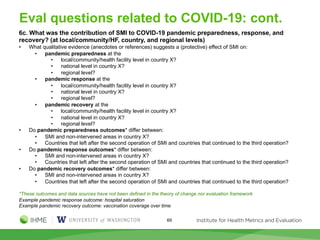
• What qualitative evidence (anecdotes or references) suggests an effect of SMI on health systems
performance?
• What evidence suggests that SMI interventions influenced performance during the system stress of the
COVID-19 pandemic?
• What qualitative evidence suggests SMI interventions have been operationalized/integrated to health
systems?
• What evidence suggests SMI interventions will continue to be funded through national spending or other
sources?
• Which SMI interventions have been operationalized and/or funded in countries that left SMI after the
second operation?
• What is the performance of MNCH outcomes (indicator Y in country X) in these cases?*
* We expect data may not be available to address these questions
5. What components of SMI influenced whether outcomes were achieved or not
according to stakeholders?
• How did component V influence (or not) outcome W according to stakeholder Z?
* We need to define the relevant list of components V
• regional model
• policy dialogue model
• RBF model
• technical assistance/coaching/mentoring
• implementation science
• responsiveness to context
• focus on local/community/facility level
• use of evidence
• external evaluation
72](https://image.slidesharecdn.com/smisteeringcommittee21mar2023-updated7june2023-230629010052-e15f43f0/85/Salud-Mesoamerica-Initiative-Mixed-Methods-Evaluation-Plan-72-320.jpg)
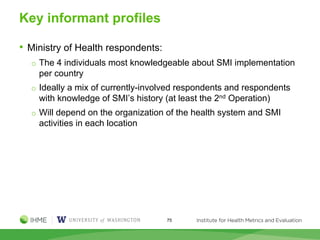
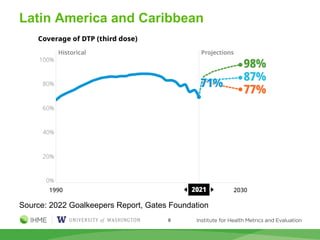
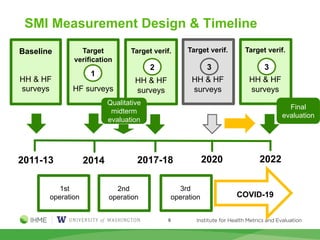
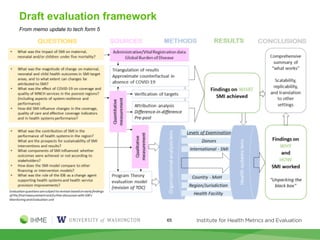
The Salud Mesoamerica Initiative (SMI) evaluation plan, dated March 21, 2023, aims to assess the project's impact on health systems through mixed methods, including quantitative and qualitative measurements. Key aspects include addressing the effects of COVID-19 on health service utilization and identifying the initiative's contributions to maternal and child health outcomes in the region. The evaluation emphasizes the importance of understanding sustainability, adaptation, and the mechanisms of change facilitated by SMI amidst global health challenges.






















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)












