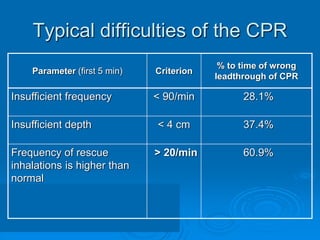
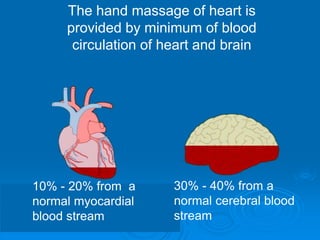
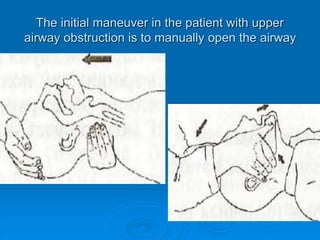
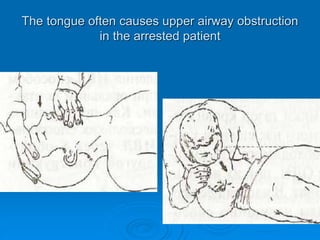
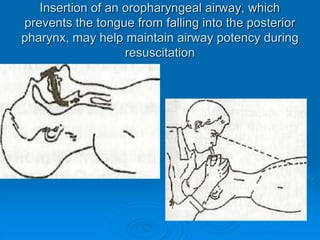
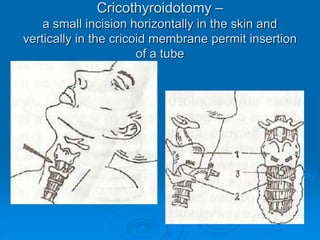
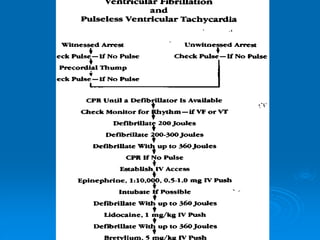
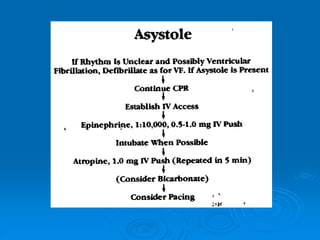
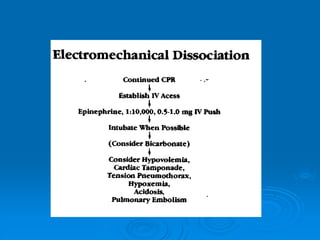
This document discusses cardiopulmonary resuscitation (CPR) and the classification and treatment of terminal patients. It covers the reversible stages of dying, defines clinical death as the cessation of circulation and breathing, and notes the timeframes for tissue survival without circulation. It describes the types of cardiac arrest and the basic ABC therapy approach. The document outlines techniques for CPR including chest compressions, ventilation, medications like epinephrine, and airway management methods. It discusses challenges with CPR delivery and notes recommendations to minimize interruptions in compressions.