Downloaded 36 times
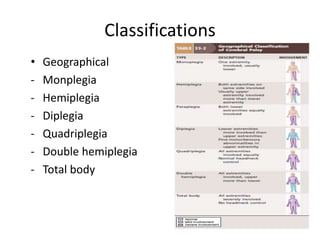
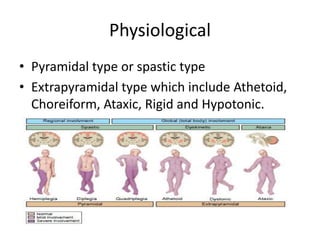




Cerebral palsy is a heterogeneous disorder of movement and posture caused by a non-progressive brain injury early in development. It presents with a wide variety of motor impairments and can be classified anatomically (e.g. hemiplegia) or physiologically (e.g. spastic, athetoid). Risk factors include prenatal, perinatal, and postnatal insults. Treatment involves both non-operative measures like medication, bracing, and physical therapy as well as operative interventions like tendon lengthening and osteotomies to prevent or treat deformities when they interfere with function. Prognosis depends on the extent and location of brain injury.






































![CP-1[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cp-11-240131015513-63dc9ac0-thumbnail.jpg?width=640&height=640&fit=bounds)




























