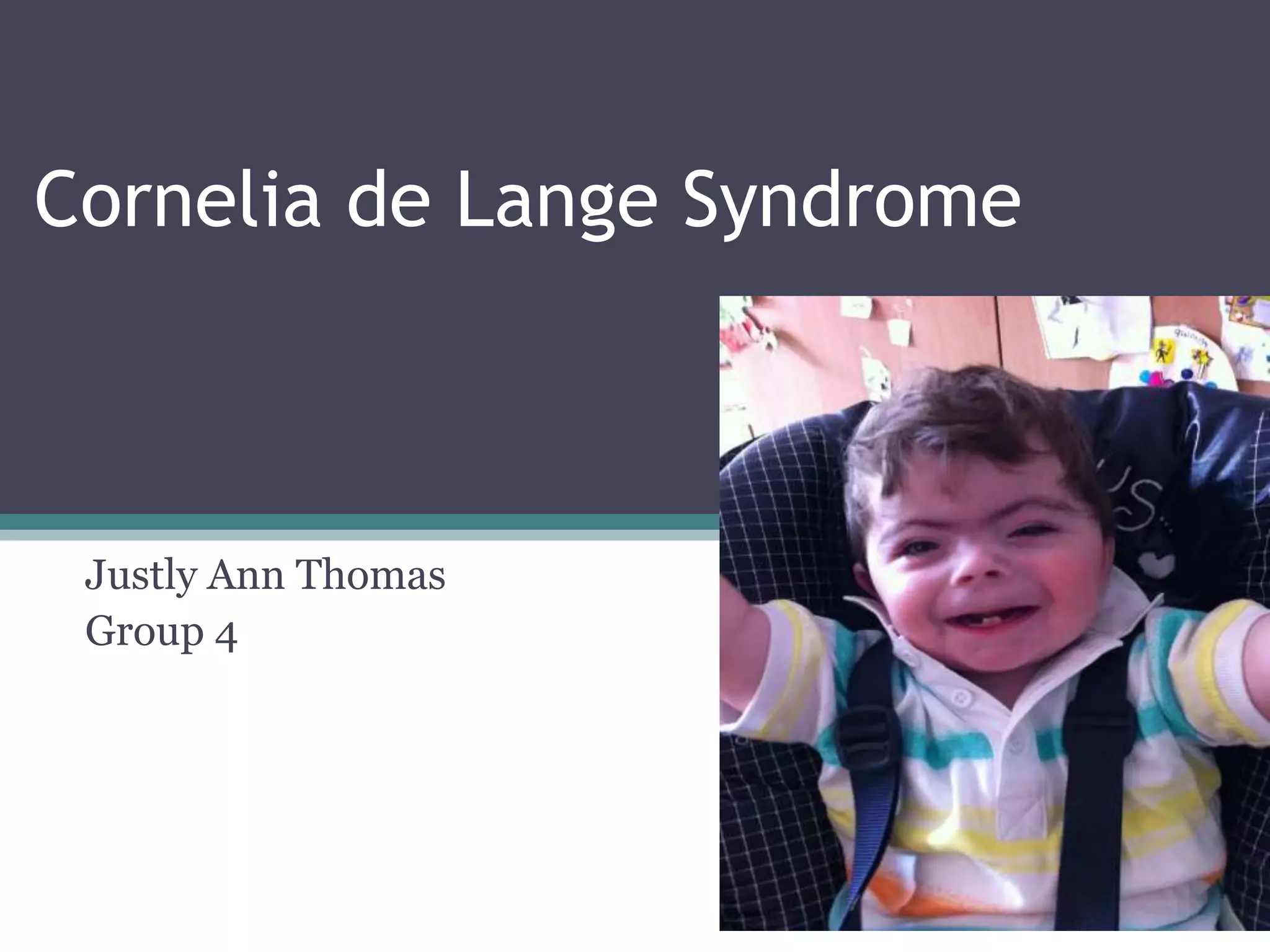
Cornelia de Lange Syndrome (CdLS) is a genetic disorder characterized by distinctive facial features, growth deficiencies, and malformations of the limbs and organs. It is caused by mutations in structural components of the cohesin complex and has an incidence of 1 in 10,000-50,000 live births. Clinical features include microcephaly, short stature, intellectual disability, and gastrointestinal issues. Diagnosis is made clinically or through genetic testing, and management requires a multidisciplinary approach including various therapies and treatments for associated health problems.