4. 382,87981,84471,05184,40791,568107,137Cash and marketable
securities2,5872,1011,5563,1525,9445,9048,55310,0979,2435,7
266,0789,7539,0359,75212,083Current
assets11,55910,1778,79910,81913,33114,01418,45821,98222,07
019,50919,49921,85221,83622,48226,863Total
assets24,34823,02121,96223,86927,48631,60437,93344,95643,1
2845,81950,82352,39757,17061,73768,371Long term
debt2,0592,7102,3532,7132,1112,1572,1371,7521,3361,1374,55
36,5397,0687,0847,103Stockholders'
equity8,5687,3626,0787,5459,83812,26914,86018,49321,52922,
72823,23822,69014,75315,57421,659Senior debt
ratingAABBB+BBB+A-AAA-AA-AAAAAA-AAAACapital
expenditures2,7682,1622,6492,3333,5153,7373,3533,6744,7126,
6957,1635,7235,6976,7148,310Financial ServicesCash and
equivalents5091,2341,3762,1683,1753,1822,5551,739Total
sales8,09610,25313,26715,80616,23515,72516,95321,302Stock
price-
high$3.97$2.89$4.63$7.79$8.56$9.85$15.88$28.16$27.50$28.3
1$24.56$18.88$24.44$33.06$35.06Stock price-
low$2.01$1.75$1.85$3.81$5.50$6.69$8.96$14.22$19.03$20.69$
12.50$11.69$13.88$21.50$25.63Stock price-
close$2.22$1.86$4.32$7.06$7.60$9.67$14.06$18.84$25.25$21.8
1$13.31$14.06$21.44$32.25$27.88Shares outstanding, year
end1,085.21,085.21,085.31,098.01,116.61,116.61,073.61,015.09
81.6945.6946.2966.6979.0998.01,023.0Sources: annual reports,
Compustat, S&P Bond Record, casewriter estimates.1) Ford's
financial statistics presented above are for the automotive
operations only, except for the Financial Services lines as
noted. The stockholholders' equity account is for the entire
consolidated company, and thus may not be comparable to the
stockholders' equity accounts of GM and Chrysler, which were
taken from the equity method statements of their respective
annual reports (see footnote on the equity method in Exhibit 8).
Exhibit 8Exhibit 8 Historical Statements of Earnings for
Chrysler with CFC and Car Rental Operations on an Equity
Basis (in millions, except share price data)
5. (1)19801981198219831984198519861987198819891990199119
9219931994Sales of manufactured
products8,6009,97210,04513,24019,57321,25522,58626,27730,7
9031,03926,96526,70733,40941,24749,534Equity in earnings of
unconsolidated
subsids.(67)(56)(6)91126256270349336353292288131187237In
terest and other
income601020194212163238833026220323Total
Revenues8,5339,97610,04913,35119,71821,55322,97726,63231,
15831,43027,34027,02533,56641,65450,094Cost of goods
sold8,5848,9158,58510,85415,52817,46818,63521,30225,90126,
69123,37823,51927,42432,06637,485Depreciation of property
and
equipment26123319618327226423746458162864466780285391
2Amortization of special
tools306218237273283213307412540620617644641671961Selli
ng and administrative
expenses5565986707769881,1441,3771,6341,7481,8752,0172,1
352,4672,6193,146Pension
expense293288272255267220236470576544531796832749704N
onpension postretirement benefit
expense12681368762828Interest
expense27626215882(51)(125)32170150929107279240361228A
sset sales, investments,
restructurings224(144)(85)(503)(101)(205)(142)(265)Total
Expenses10,27610,51410,11812,64717,28719,18420,68024,4522
9,53730,86527,19327,83532,63237,81644,264Earnings Before
Taxes(1,743)(538)(69)7042,4312,3692,2972,1801,621565147(81
0)9343,8385,830Provision for income
taxes2917040293473590889061224279(272)4291,4232,117Chan
ge in accounting principles (2)(41)(36)(257)218(4,966)Net
Earnings
(Loss)(1,772)(555)(69)3021,4971,6341,3891,2901,05035968(79
5)723(2,551)3,713Selected Market InformationSenior debt
ratingNRNRNRBBBBBBBBBBBBBBBBBBBBBB-BB-
B+BBBBBB+Stock price-
6. high$5.17$3.39$8.28$15.83$15.00$20.89$31.42$48.00$27.88$2
9.63$20.38$15.88$33.88$58.38$63.50Stock price-
low$1.83$1.33$1.56$6.22$9.28$13.28$18.11$19.63$20.50$18.1
3$9.13$9.75$11.50$31.75$43.13Stock price-
close$2.17$1.50$7.89$12.28$14.22$20.72$24.67$22.13$25.75$
19.00$12.63$11.75$32.00$53.25$44.88Shares outstanding, year
end150.69164.55178.82274.08273.31227.80216.69221.22233.10
223.10224.80292.30295.90353.73355.06Sources: annual
reports, S&P Bond Record, and casewriter estimates.1) The
historical financial statements for Chrysler were taken from
statements prepared using the equity method rather than the
consolidated method. In the equity method, the financial
statements show accounts from the core business entity and then
add a summary account for the net effect of affiliates and
subsidiaries. For example, on the balance sheet, the asset
"Investments in unconsolidated subsidiaries and affiliates"
represents the sum of the assets (net of liabilities) of the
subsidiaries. On the income statement, the combined earnings of
subsidiaries and affiliates are added in one line called "Equity
in earnings of unconsolidated subsidiaries." In consolidated
statements, the individual subsidiary accounts are merged into
the parent accounts on a line-by-line basis.2) The large charge
in 1993 reflects new SFAS rule regarding accounting for
postretirement benefits other than pensions, net of a tax benefit
estimate.
Exhibit 9Exhibit 9 Historical Balance Sheets for Chrysler with
CFC and Car Rental Operations on an Equity Basis (in
millions)Assets:198019811982198319841985198619871988198
919901991199219931994Cash and
equivalents104121109112751482851,5421,5059591,4911,5052,
0093,7774,972Marketable
securities1942837889581,6252,6502,3948681,4461,1811,47369
69597072,643Total cash and marketable
securities2984048971,0701,7002,7982,6792,4102,9512,1402,96
42,2012,9684,4847,615Accounts receivable - trade and other
(net)4764302482913322083725781,137993695626936805459In
7. ventories1,9161,6001,1331,3011,6261,8631,6992,5522,9712,53
62,6092,4352,3302,4832,645Prepaid taxes, pension, and other
expenses17216791923224466136316645154175015437131,272P
roperty and
equipment1,7191,6491,6952,1362,6293,2774,3145,8496,2246,1
766,3937,2848,0978,82010,347Special
tools8017987789191,0841,3621,8042,4632,4652,4872,5072,640
2,8963,4553,643Investments in unconsolidated
subsidiaries1,0851,0591,2388621,2412,0702,2442,7212,8142,94
73,2413,7723,6873,6853,642Intangible
assets3872,1372,5434,2644,7424,5504,1363,8821,781Deferred
tax assets7411,4803,6421,951Other
assets1511621831011285822876047371,5739537945712,0514,7
22Total
Assets6,6186,2706,2636,7729,06212,60614,39919,94522,50623,
63124,52125,54427,64434,02038,077Liabilities:Accounts
payable1,1791,0238981,6292,3232,5052,9583,7224,3463,5753,9
844,3575,0136,0747,403Current portion of long-term
debt36128115445150297202285217283279745142499327Accru
ed liabilities and
expenses1,3639609166271,7431,9281,9612,6313,0473,2383,020
3,5923,7934,4225,333Long-term
debt2,4832,0592,1481,1047602,3662,3343,3333,3292,9653,944
3,6723,6432,2812,097Accrued noncurrent employee
benefits3536666369873622982907497132,9713,7534,3844,1871
0,5628,547Other noncurrent
liabilities2222783524324976056611,5262,0932,8612,6922,6853
,3283,3463,676Deferred income
taxes197223169178223927121,1961,179505Total
Liabilities6,1585,4905,2735,4085,7578,3919,11813,44214,9241
6,39817,67219,43520,10627,18427,383Shareholders'
Equity:Preferred stock5641,3191,321221222Common
stock419460500122124153229245245245245312312364364Add
itional paid-in
capital6926936932,2762,3251,9431,8672,3742,3762,3692,2912,
9053,6575,5335,536Retained
8. earnings(1,215)(1,692)(1,524)(1,255)9212,1533,5044,5815,3585
,2294,8133,3853,9241,1705,006Treasury stock - at
cost(65)(34)(319)(697)(397)(610)(500)(493)(357)(233)(214)Tot
al Shareholders'
Equity4607809901,3643,3054,2155,2816,5037,5827,2336,8496,
1097,5386,83610,694Total Liabilities and Shareholders'
Equity6,6186,2706,2636,7729,06212,60614,39919,94522,50623,
63124,52125,54427,64434,02038,077Sources: annual reports
and casewriter estimates.
Exhibit 10Exhibit 10 Historical Statements of Cash Flows for
Chrysler with CFC and Car Rental Operations on an Equity
Basis (in millions)Cash Flows from Operating
Activities:19801981198219831984198519861987198819891990
1991199219931994Net earnings
(loss)(1,772)(555)(69)3021,4971,6341,3891,2901,05035968(795
)723(2,551)3,713Adjustments to get to operating cash
flow:Depreciation and
Amortization5674514324575544765448761,1211,2481,2611,311
1,4431,5241,873Provision for restructuring
charges150929(101)Equity in earnings of unconsolidated
subs.67566(91)(126)(256)(270)(349)(336)(353)(292)(288)(131)(
187)(237)Plant capacity adjustment(391)Deferred income
taxes22546685663473(135)55(288)2298031,065Gain on sales of
auto assets and
investments(16)(126)(539)(205)(142)(265)Cumulative effect of
chng. in acctg. principles257(218)4,966Change in accounts
receivable1344784(165)390(445)12011369(300)131345Change
in
inventories(42)316332(212)(594)102163(493)(271)(26)(87)1741
59(171)(201)Change in prepaid expenses and other
assets(148)138(331)80(73)2574(1,587)(2,095)Change in
accounts payable and other
liabs.504(514)451,0241,029310487310900(874)(372)963953365
2,856Change in noncurrent assets and
liabilities3381(49)(41)339(351)(364)Dividends/earnings
received from
9. subsidiary6280100350Other(48)(6)216829041191572321993011
98199181224215Net Cash Provided by Operating
Activities(525)2558022,1213,2732,9702,4912,6932,3841,2101,1
201,0312,9713,2527,534Cash Flows from Investing
Activities:Purchase (sale) of non-core assets
(1)269(672)(555)Purchases of marketable
securities(2,598)(4,357)(6,779)(6,442)(14,188)(3,149)(3,412)Sa
les and maturities of marketable
securities3116302,0214,6216,4877,21713,9253,4011,463Procee
ds from sale of assets
(2)(39)(29)(185)245(252)(519)(15)(131)59882010021546162Ne
t expenditures for property and
equipment(319)(122)(85)(634)(760)(1,043)(1,287)(1,234)(987)(
932)(1,034)(1,482)(1,374)(1,738)(2,611)Expenditures for
special
tools(395)(214)(227)(415)(447)(492)(749)(655)(557)(651)(663)
(708)(872)(1,234)(1,177)Other(43)(44)1(12)13(2)(35)138(315)(
214)(121)(209)(13)77Net Cash Used in Investing
Activities(796)(409)(227)(816)(1,459)(2,713)(1,742)(1,980)(1,9
83)(1,036)(1,383)(1,436)(2,503)(2,272)(5,598)Cash Flows from
Financing Activities:Change in Short-term
debt5013(24)282(354)29(113)(10)16(9)12249(165)1440Long-
term
borrowings1,157432112201031,8341381,082118251,254183392
32Payments on long-term
borrowings(64)(185)(70)(1,583)(508)(65)(141)(815)(323)(247)(
343)(37)(497)(1,021)(412)Net common and preferred stock
proceeds11163(315)(843)(291)(391)3858361,952Dividends
paid(117)(121)(115)(153)(214)(225)(268)(269)(169)(225)(281)(
399)Other213(1)4(5)(23)(221)3184810128Net Cash Provided by
Financing
Activities1,144261(82)(1,133)(1,182)839(556)(353)(437)(720)7
9541936788(741)Change in cash and cash
equivalents(177)1074931726321,096193360(36)(546)53214504
1,7681,1951) Reflects purchase of Chrysler Defense in 1982,
Gulfstream Aerospace in 1985, and AMC and ESI in 1987.2)
10. Reflects proceeds from sale of Gulfstream Aerospace in
1990.Sources: annual reports and casewriter estimates.
Exhibit 11Exhibit 11 Chrysler Projected Income Statements,
1994-1998E (in millions)19941995E1996E1997E1998ESales of
manufactured products49,53453,23956,03759,49756,894Equity
in earnings of unconsolidated
subsidiaries237164200200200Interest and other
income323191300300300Total
Revenues50,09453,59456,53759,99757,394Cost of goods
sold37,48540,03442,19644,78443,325Depreciation of property
and equipment9129209801,0501,010Amortization of special
tools9611,0801,1501,2001,160Selling and administrative
expense3,1463,2803,4743,6293,647Pension
expense704650630610590Nonpension postretirement benefit
expense828750740730730Interest
expense228228210205190Total
Expenses44,26446,94249,38052,20850,652Earnings Before
Taxes5,8306,6527,1577,7896,742Provision for income
taxes2,1172,5942,7913,0382,630Net
Income3,7134,0584,3664,7514,112
Exhibit 12Exhibit 12 Chrysler Projected Cash Flows, 1994-
1998E (in millions, except per share
data)19941995E1996E1997E1998ENet
Income3,7134,0584,3664,7514,112Depreciation9129209801,050
1,010Amortization of special
tools9611,0801,1501,2001,160Equity in unconsolidated
subsidiaries(237)(164)(200)(200)(200)Deferred taxes
(1)1,0659791,0381,1211,121Change in net working
capital1,1200000Total
Sources7,5346,8737,3347,9227,203Capital
expenditures3,7883,2003,1003,1003,100Debt
payments37019030350350Stock repurchases01,000000Net
equity interest sales1,7200000Total
Uses5,8784,3903,1303,4503,450Net Cash
Flow1,6562,4834,2044,4723,753Net cash flow per
share4.066.2710.8411.539.67Dividends on common and
11. preferred399660726798800Excess Cash
Flow1,2571,8233,4783,6742,953Source: compiled from Morgan
Stanley research reports.1) The deferred tax add-back represents
the amount by which income taxes for financial reporting
exceed the cash outflow computed for tax accounting.
Exhibit 13Exhibit 13 Betas for the Big Three, April,
1995Chrysler1.30General Motors1.15Ford1.15Source: Value
Line
Exhibit 14Exhibit 14 Financial Market Data, April 1995I.
Treasury Yields90 day5.818%Six months6.075One
year6.316Five years6.946Ten years7.112Thirty years7.395II.
Corporate Borrowing RatesLong Term Bond
YieldsAaa8.08%Aa8.19A8.28Baa8.65Sources: Federal Reserve
Bulletin, Bloomberg, Value Line
· My Bookshelf
· TOC/Annotation menu
· Downloads
· Print
· Search
· Profile
· Help
Chapter 18 Partners HealthCare System
Previous section
Next section
18 Partners HealthCare System
Thomas H. Davenport
Partners HealthCare System (Partners) is the single largest prov
ider of healthcare in the Boston area. It consists of 12 hospitals,
with morethan 7,000 affiliated physicians. It has 4 million outp
atient visits and 160,000 inpatient admissions a year. Partners is
a nonprofitorganization with almost $8 billion in revenues, and
it spends more than $1 billion per year on biomedical research.
It is a major teachingaffiliate of Harvard Medical School.
Partners is known as a “system,” but it maintains substantial aut
onomy at each of its member hospitals. While some information
12. systems(the electronic medical record, for example) are standar
dized across Partners, other systems and data, such as patient sc
heduling, arespecific to particular hospitals. Analytical activitie
s also take place both at the centralized Partners level and at ind
ividual hospitals such asMassachusetts General Hospital (MGH)
and Brigham and Women’s Hospital (usually described as “the
Brigham”). In this chapter, bothcentralized and hospital-
specific analytical resources are described. The focus for hospit
al-
specific analytics is the two major teachinghospitals of Partners
—MGH and the Brigham—
although other Partners hospitals also have their own analytical
capabilities and systems.
Centralized Data and Systems at Partners
The basis of any hospital’s clinical information systems is the cl
inical data repository, which contains information on all patient
s, theirconditions, and the treatments they have received. The in
patient clinical data repository for Partners was initially implem
ented at theBrigham during the 1980s. Richard Nesson, the Brig
ham and Women’s CEO, and John Glaser, the hospital’s chief in
formation officer,initiated an outpatient electronic medical reco
rd (EMR) at the Brigham in 1989.1 This EMR contributed outpa
tient data to the clinical datarepository. The hospital was one of
the first to embark on an EMR, though MGH had begun to deve
lop one of the first full-function EMRs asearly as 1976.
A clinical data repository provides the basic data about patients.
Glaser and Nesson came to agree that in addition to a repositor
y and anoutpatient EMR, the Brigham—
and Partners after 1994, when Glaser became its first CIO—
needed facilities for doctors to input onlineorders for drugs, test
s, and other treatments. Online ordering (called CPOE, or Comp
uterized Provider Order Entry) would not only solvethe time-
honored problem of interpreting poor physician handwriting, but
could also, if endowed with a bit of intelligence, check whether
aparticular order made sense or not for a particular patient. Did
a prescribed drug comply with best-
13. known medical practice, and did thepatient have any adverse rea
ctions in the past to it? Had the same test been prescribed six ti
mes before with no apparent benefit? Was thespecialist to whom
a patient was being referred covered by his or her health plan?
With this type of medical and administrative knowledgebuilt int
o the system, dangerous and time-
consuming errors could be prevented. The Brigham embarked on
its CPOE system in 1989.
Nesson and Glaser knew that there were other approaches to red
ucing medical error than CPOE. Some provider institutions, suc
h asIntermountain Healthcare in Utah, were focused on close ad
herence by physicians to well-
established medical protocols. Others, like KaiserPermanente in
California and the Cleveland Clinic, combined insurance and m
edical practices in ways that incented all providers to workjointl
y on behalf of patients. Nesson and Glaser admired those approa
ches, but felt that their impact would be less in an academic me
dicalcenter such as Partners, where physicians were somewhat a
utonomous, and individual departments prided themselves on th
eir separatereputations for research and practice innovations. Co
mmon, intelligent systems seemed like the best way to improve
patient care atPartners.
In 1994, when the Brigham and Mass General combined as Partn
ers HealthCare System, there was still considerable autonomy fo
rindividual hospitals in the combined organization. However, fr
om the onset of the merger, the two hospitals agreed to use a co
mmonoutpatient EMR called the longitudinal medical record (L
MR) and a CPOE system, both of which were developed at the B
righam. This waspowerful testimony in favor of the LMR and C
POE systems, since there was considerable rivalry between the t
wo hospitals, and MassGeneral had its own EMR.
Perhaps the greatest challenge was in getting the extended netw
ork of Partners-
affiliated physicians up on the LMR and CPOE. Thephysician n
etwork of more than 6,000 practicing generalist and specialist p
hysician groups was scattered around the Boston metropolitanar
14. ea, and often operated out of their own private offices. Many lac
ked the IT or telecom infrastructures to implement the systems
on theirown, and implementation of an outpatient EMR cost abo
ut $25,000 per physician. Yet full use of the system across Partn
ers-
affiliatedproviders was critical to a seamless patient experience
across the organization.
Glaser and the Partners information systems (IS) organization w
orked diligently to spread the LMR and CPOE to the growing nu
mber ofPartners hospitals and to Partners-
affiliated physicians and medical practices. To assist in bringin
g physicians outside the hospitals onboard, Partners negotiated
payment schedules with insurance companies that rewarded phy
sicians for supplying the kind of informationavailable from the
LMR and CPOE. By 2007, 90% of Partners-
affiliated physicians were using the systems, and by 2009, 100%
were. By2009, more than 1,000 orders per hour were being ente
red through the CPOE system across Partners.
The combination of the LMR and the CPOE proved to be a powe
rful one in helping to avoid medical error. Adverse drug events,
or the useof the wrong drug for the condition or one that caused
an allergic reaction in the patient, typically were encountered b
y about 14 of every1,000 inpatients. At the Brigham before LM
R and CPOE, the number was about 11. After the widespread im
plementation of these systems atBrigham and Women’s, there w
ere just above five adverse drug events per 1,000 inpatients—
a 55% reduction.
Managing Clinical Informatics and Knowledge at Partners
The Clinical Informatics Research & Development (CIRD) grou
p, headed by Blackford Middleton, is one of the key centralized
resources forhealthcare analytics at Partners. Many of CIRD’s st
aff, like Middleton, have multiple advanced degrees; Middleton
has an MD, a Master ofPublic Health degree, and a Master of Sc
ience in Health Services Research.
The mission of CIRD is
to improve the quality and efficiency of care for patients at Part
15. ners HealthCare System by assuring that the most advancedcurr
ent knowledge about medical informatics (clinical computing) is
incorporated into clinical information systems at PartnersHealt
hCare.2
CIRD is part of the Partners IS organization. It was CIRD’s role
to help create the strategy for how Partners used information sy
stems inpatient care, and to develop both production systems ca
pabilities and pilot projects that employ informatics and analyti
cs. CIRD’s work hadplayed a substantial role in making Partner
s a worldwide leader in the use of data, analysis, and computeri
zed knowledge to improvepatient care. CIRD also has had sever
al projects funded by U.S. government health agencies to adapt
some of the same tools andapproaches it developed for Partners
to the broader healthcare system.
One key function of CIRD was to manage clinical knowledge, a
nd translate healthcare research findings into daily medical prac
tice atPartners. In addition to facilitating adoption of the LMR a
nd CPOE, Partners faced a major challenge in getting control of
the clinicalknowledge that was made available to care provider
s through these and other systems. The “intelligent CPOE” strat
egy demanded thatknowledge be online, accessible, and easily u
pdated so that it could be referenced by and presented to care pr
oviders in real-
timeinteractions with patients. There were, of course, a variety
of other online knowledge tools, such as medical literature searc
hing, available toPartners personnel; in total they were referred
to as the “Partners Handbook.” At one point after use of the CP
OE had become widespreadat Brigham and Women’s, a compari
son was made between online usage of the Handbook and usage
of the knowledge base from orderentry. There were more than 1
3,000 daily accesses through the CPOE system at the Brigham a
lone, and only 3,000 daily accesses of theHandbook by all Partn
ers personnel at all hospitals. Therefore, there was an ongoing e
ffort to ensure that as much high-
quality knowledgeas possible made it into the CPOE.
The problem with knowledge at Partners was not that there wasn
16. ’t enough of it; indeed, the various hospitals, labs, departments,
andindividuals were overflowing with knowledge. The problem
was how to manage it. At one point, Tonya Hongsermeier, a phy
sician with anMBA degree who was charged with managing kno
wledge at Partners, counted the number of places around Partner
s where there wassome form of rule-
based knowledge about clinical practice that was not centrally
managed. She found about 23,000 of them. The knowledgewas c
ontained in a variety of formats: paper documents, computer “sc
reen shots,” process flow diagrams, references, and data or repo
rtson clinical outcomes—
all in a variety of locations, and only rarely shared.
Hongsermeier set out to create a “knowledge engineering and m
anagement” factory that would capture the knowledge at Partner
s, put it ina common format and central repository, and make it
available for CPOE and other online systems. This required not
only a new computersystem for holding the thousands of rules t
hat constituted the knowledge, but an extensive human system f
or gathering, certifying, andmaintaining the knowledge. It consi
sted of the following roles and organizations:
• A set of committees of senior physicians who oversaw clinical
practice in various areas, such as the Partners Drug TherapyCo
mmittee, which reviewed and sanctioned the knowledge as corre
ct or best known practice
• A group of subject matter experts who, using online collaborat
ion systems, debated and refined knowledge such as the best dru
g fortreating high cholesterol under various conditions, or the b
est treatment protocol for diabetes patients
• A cadre of “knowledge editors” who took the approved knowle
dge from these groups and put it into a rule-
based form that wouldbe accepted by the online knowledge repo
sitory
High Performance Medicine at Partners
Glaser and Partners IS had always had the support of senior Part
ners executives, but for the most part their involvement in the a
ctivitiesdesigned to build Partners’ informatics and analytics ca
17. pabilities was limited to some of the hospitals and those physici
an practices thatwanted to be on the leading edge. Then Jim Mo
ngan moved from being president of MGH (a role he had occupi
ed since 1996, shortly afterthe creation of Partners) to being CE
O of Partners overall in January 2003. Not since Dick Nesson ha
d Glaser had such a strong partner inthe executive suite.
Mongan had come to appreciate the value of the LMR and CPO
E, and other clinical systems, while he headed Mass General. B
ut when hecame into the Partners CEO role, with responsibility
over a variety of diverse and autonomous institutions, he began
to view it differently.Mongan said:
So when I was preparing to make the move to Partners, I began t
o think about what makes a health system. One of the keys that
would unite us was the electronic record. I saw it as the connect
ive tissue, the thing we had in common, that could help us get a
handle on utilization, quality, and other issues.
Together Mongan and Glaser agreed that while Partners already
had strong clinical systems and knowledge management compar
ed toother institutions, a number of weaknesses still needed to b
e addressed (most importantly that the systems were not univers
ally usedacross Partners care settings), and steps needed to be ta
ken to get to the next level of capability. Working with other cli
nical leaders atPartners, they began to flesh out the vision for w
hat came to be known as the High Performance Medicine (HPM)
initiative, which took placebetween 2003 and 2009.
Glaser commented on the process the team followed to specify t
he details of the HPM initiative:
Shortly after he took the reins at Partners, however, Jim had a cl
ear idea on where he wanted this to go. To help refine that visio
n,several of us went on a road trip, to learn from other highly in
tegrated health systems such as Kaiser, Intermountain Healthcar
e,and the Veterans Administration about ways we might bring th
e components of our system closer together.
Mongan concluded:
We also were working with a core team of 15-
20 clinical leaders and eventually came up with a list of seven o
18. r eight initiatives,which then needed to be prioritized. We did a
“Survivor”-
style voting process, to determine which initiatives to “kick off
the island.”That narrowed down the list to five Signature Initiati
ves.
The five initiatives consisted of the following specific programs
, each of which was addressed by its own team:
• Creating an IT infrastructure—
Much of the initial work of this program had already been done;
it consisted of the LMR and theCPOE, which was extended to t
he other hospitals and physician practices in the Partners networ
k and maintained. This project alsoaddressed patient data qualit
y reporting, further enhancement of knowledge management pro
cesses, and a patient data portal togive patients access to their o
wn health information.
• Enhancing patient safety—
The team addressing patient safety issues focused on four specif
ic projects: 1) providing decisionsupport about what medication
s to administer in several key areas, including renal and geriatri
c dosing; 2) communicating “clinicallysignificant test results,”
particularly to physicians after their patients have left the hospit
al; 3) ensuring effective flow of informationduring patient care t
ransitions and handoffs in hospitals and after discharge; 4) prov
iding better decision support, patient education,and best practic
es and metrics for anticoagulation management.
• Uniform high quality—
This team addressed quality improvement in the specific domain
s of hospital-
based cardiac care,pneumonia, diabetes care, and smoking cessa
tion; it employed both registries and decision support tools to d
o so.
• Chronic disease management—
The team addressing disease management focused on prevention
of hospital admission byidentifying Partners patients who were
at highest risk for hospitalization, and then developed health co
aching programs to addresspatients with high levels of need, for
19. example, heart failure patients; the team also pulled together a
new database of informationabout patient wishes about end-of-
life decisions.
• Clinical resource management—
At Jim Mongan’s suggestion, this team focused on how to lower
the usage of high-cost drugs andhigh-
cost imaging services; it employed both “low-
tech” methods (e.g., chart reviews) and “high-
tech” approaches (e.g., a datawarehouse making transparent phy
sicians’ imaging behaviors relative to peers) to begin to make u
se of scarce resources moreefficiently.
Overall, Partners spent about $100 million on HPM and related
clinical systems initiatives, most of which were ultimately paid
for by thePartners hospitals and physician practices that used th
em. To track progress, a Partners-
wide report, called the HPM Close, was developedthat shows cu
rrent and trend performance on the achievement of quality, effic
iency, and structural goals. The report was publishedquarterly t
o ensure timely feedback for measuring performance and suppor
ting accountability across Partners.
New Analytical Challenges for Partners
Partners had made substantial progress on many of the basic app
roaches to clinical analytics, but there were many other areas at
theintersection of health and analytics that it could still address.
One was the area of personalized genetic medicine—
the idea that patientswould someday receive specific therapies b
ased on their genomic, proteomic, and metabolic information. P
artners had created the i2b2(Informatics for Integrating Biology
and the Bedside), a National Center for Biomedical Computing
that was funded by the NationalInstitutes of Health. John Glaser
was co-
director of i2b2 and developed the IT infrastructure for the Part
ners Center for PersonalizedGenetic Medicine. One of the many
issues these efforts addressed in personalized genetic medicine
was how relevant genetic informationwould be included in the L
MR.
20. Partners was also attempting to use clinical information for post
market surveillance—
the identification of problems with drugs and medicaldevices in
patients after they have been released to the market. Some Partn
ers researchers had identified dangerous side effects fromcertain
drugs through analysis of LMR data. Specifically, research scie
ntist John Brownstein’s analyses suggested that the level of pati
entswith heart attack admissions to Mass General and the Brigh
am had increased 18% beginning in 2001 and returned to its bas
eline level in2004, which coincided with the timeframe for the b
eginning and end of Vioxx prescriptions. Thus far the identifica
tion of problems hadtaken place only after researchers from oth
er institutions had identified them, but Partners executives belie
ved it had the ability to identifythem at an earlier stage. The ins
titution was collaborating with the Food and Drug Administratio
n and the Department of Defense toaccelerate the surveillance p
rocess. John Glaser noted:
I don’t know that we’ll get as much specificity as might be need
ed to really challenge whether a drug ought to be in a market, b
ut Ialso think it’s fairly clear that you can be much faster and in
volve much fewer funds, frankly, to do what we would call the “
canaryin the mine” approach.3
Partners was also focused on the use of communications technol
ogies to improve patient care. Its Center for Connected Health,
headed byDr. Joe Kvedar, developed one of the first physician-
to-
physician online consultation services in an academic medical s
etting. The Center wasalso exploring combinations of remote m
onitoring technologies, sensors (for example, pill boxes that kno
w whether today’s dosage hasbeen taken), and online communic
ations and intelligence to improve patient adherence to medicati
on regimes, engagement in personalhealth, and clinical outcome
s.
In the clinical knowledge management area, Partners had done a
n impressive job of organizing and maintaining the many rules a
ndknowledge bases that informed its “intelligent” CPOE system.
21. However, it was apparent to Glaser, Blackford Middleton, and
TonyaHongsermeier—
and her successor as head of knowledge management, Roberto R
ocha—
that it made little sense for each medicalinstitution to develop it
s own knowledge base. Therefore, Partners was actively engage
d in helping other institutions with the managementof clinical k
nowledge. Middleton (the principal investigator), Hongsermeier,
Rocha, and at least 13 other Partners employees were involvedi
n a major Clinical Decision Support Consortium project funded
by the U.S. Agency for Healthcare Research and Quality. The c
onsortiuminvolved a variety of other research institutions and h
ealthcare companies, and was primarily focused on finding ways
to make clinicalknowledge widely available to healthcare provi
ders through EMR and CPOE systems furnished by leading vend
ors.
Despite all these advances, not all Partners executives and physi
cians had fully bought into the vision of using smart informatio
n systems toimprove patient care. Some found, for example, the
LMR and CPOE to be invasive in the relationship of doctor and
patient. A seniorcardiologist at Brigham and Women’s, for exa
mple, argued in an interview [with the author] that:
I have a problem with the algorithmic approach to medicine. Pe
ople end up making rote decisions that don’t fit the patient, and
itcan also be medically quite wasteful. I don’t have any choice h
ere if I want to write prescriptions—
virtually all of them are doneonline. But I must say that I am ge
tting alert fatigue. Every time I write a prescription for nitrogly
cerine, I am given an alert thatasks me to ensure that my patient
isn’t on Viagra. Don’t you think I know that at this point? As f
or online treatment guidelines, Ibelieve in them up to a point. B
ut once something is in computerized guidelines it’s sacrosanct,
whether or not the data arelegitimate. Recommendations should
be given with notification of how certain we are about them....
Maybe these things are moreuseful to some doctors than others.
If you’re in a subspecialty like cardiology you know it very well
22. . But if you are an internist, youmay have shallow knowledge, b
ecause you have to cover a wide variety of medical issues.
Many of the people involved in developing computer systems fo
r patient care at Partners regarded these as valid concerns. “Aler
t fatigue,”for example, had been recognized as a problem within
Blackford Middleton’s group for several years. They had tried t
o eliminate the moreobvious alerts, and to make changes in the
system to allow physicians to modify the types of alerts they rec
eived. There was a difficult lineto draw, however, between savi
ng physician attention and saving lives.
Centralized Business Analytics at Partners
While much of the centralized analytical activity at Partners has
been on the clinical side, the organization is also making progr
ess onbusiness analytics. The primary focus of these efforts is o
n financial reporting and analysis.
For several years, for example, Partners has employed an extern
al “software as a service” tool to provide reporting on the organ
ization’srevenue cycle. It has also developed several customized
analytics applications in the areas of cash management, underp
ayments, bad debtreserves, and charge capture. These activities
primarily took place in the Partners Revenue Finance function.
The Partners Information Systems organization is also increasin
g its focus on administrative and financial analytics. It is puttin
g in placeCompass, a common billing and administrative system
, at all Partners hospitals. At the same time, Partners has created
a set of standardprocesses for collecting, defining, and modifyi
ng financial and administrative data. Further, as one article put i
t:
At Partners, John Stone, corporate director for financial and ad
ministrative systems, is developing a corporate center of busine
ssanalytics and business intelligence. Some 12 to 14 financial e
xecutives will oversee the center, define Partners’ strategy for d
atamanagement, and determine data-
related budget priorities. “Our analysts spend the majority of th
eir time gathering, cleaning, andscrubbing administrative data a
nd less time providing value-
23. added analytics and insight into what the data is saying,” says S
tone.“We want to flip that equation so our analysts are spending
more time producing a story that goes along with the data.”4
Hospital-Specific Analytical Activities—
Massachusetts General Hospital
MGH, because it was a highly research-
driven institution, had long focused primarily on clinical resear
ch and the resulting clinicalinformatics and analytics. In additio
n to the LMR and CPOE systems used by Partners overall, MGH
researchers and staff have developed anumber of IT tools to an
alyze and search clinical data, one of which was a tool that sear
ched across multiple enterprise clinical systems,including the L
MR.
While historically, the research, clinical, information systems, a
nd the analytically focused business arms of MGH tended to ope
rate in stovepipes, the challenges of an evolving healthcare land
scape have forced a change in that paradigm. For instance, a str
ong current focus withinMGH is on how to achieve federal “mea
ningful use” reimbursement for the organization’s expenditures
on EMR. Because achievingmeaningful use objectives is predica
ted on a high level of coordination among information systems,
the physicians, and businessintelligence, people like David Y. T
ing, the associate medical director for Information Systems for
MGH and Massachusetts GeneralPhysicians Organization, and C
hris Hutchins, the director of Finance Systems and deputy CIO,
are beginning to collaborate extensively.
The HITECH/ARRA criteria for Stage 1 EMR meaningful use pr
escribe 25 specific objectives to incentivize providers to adopt a
nd useelectronic health records.5
To raise the level of EMR use by all its providers, as well as to
provide resources for the work needed to achieve that level, MG
H has arrivedat a novel funds distribution model. They determin
ed that the physicians organization will reserve a portion of the
pool of $44,000 perphysician toward IT and analytics infrastruct
ure, then distribute the remaining incentive payment across all p
roviders, proportional to theamount of data a particular physicia
24. n is charged with entering. An internal quality incentive progra
m would serve as the distributionmechanism. So, for example, if
you recorded demographics, vital signs, and smoking status for
the requisite number of patients, you wouldreceive 30% of the p
er-
physician payment from the pool. If you fulfilled all ten quality
measures, you would receive 100% of the paymentfrom the pool
. This encourages all physicians to contribute to the meaningful
use program, but it also means that no physicians will receiveth
e full amount of $44,000. The incentive from the federal govern
ment is up to $44,000 for each eligible provider who fulfills the
meaningful use criteria. MGH has examined the objectives and
broken them down into ten major pieces of patient data that phy
sicians needto record in the EMR. However, many are not releva
nt for all of its physicians. For example, a primary care physicia
n would logically entersuch data as demographics, vital signs, a
nd smoking status, but these would be less relevant for certain s
pecialists to enter.
Clearly, such a complex quality incentive model requires an unp
recedented level of analytics. Currently, Ting, Hutchins, and oth
ers at MGHare working to map the myriad clinical and finance d
ata sources that are scattered among individual departments, exi
st at a hospital sitelevel, or exist at the Partners enterprise level.
Simultaneously, they must negotiate data governance agreemen
ts even among other Partnersentities, to ensure that the requisite
data feeds from sources within Partners and pertaining to MGH
, but stored outside MGH’s physical datawarehouses, are availa
ble for MGH analytics purposes.
MGH has some experience with reimbursement metrics based on
physician behaviors, having used them in Partners Community
HealthCare, Inc. (PCHI), its physician network in the Boston ar
ea. Physician incentives have been provided through PCHI on th
e basis ofadmission rates, cost-
effective use of pharmacy and imaging services, and screening f
or particular diseases and conditions, such as diabetes. This was
also the mechanism used to encourage the adoption of the LMR
25. and CPOE systems by physicians. But MGH, like otherprovider
s, struggles with developing clear and transparent metrics across
the institution that can help to drive awareness and newbehavio
rs. If MGH could create broadly accessible metrics on individua
l physicians’ frequency of prescribing generic drugs, for exampl
e, itwould undoubtedly drive MGH’s competitive physicians to
excel in the rankings.
On the business side, MGH is trying to develop a broad set of c
apabilities in business intelligence and analytics. A BusinessInt
elligence/Performance Management group has recently been cre
ated under the direction of Chris Hutchins, deputy CIO and dire
ctor offinance systems for the Mass General Physicians Organiz
ation (MGPO). The group is generating reports on such financia
l and administrativetopics as
• Billing efficiency, claims adjudication, rejection rates, and tim
es to resolve billing accounts, both at MGH overall and across p
ractices
• Improving patient access, average wait times to see a physicia
n, and cancellation and no show rates
• Employer attrition as an MGH customer
MGH is also working with CMS on the Physician Quality Repor
ting Initiative. To combine all these measures in a meaningful f
ashion, MGPO isalso working on a balanced scorecard.6
While the current analytical activity is largely around reporting,
Hutchins plans to develop more capabilities around alerts, exce
ptionreporting, and predictive models. The MGH Physicians Or
ganization is implementing capabilities for statistical and predic
tive analytics thatwould be applied to several topics. For examp
le, one key area in which better prediction would be useful invo
lves patient volume. They arealso pursuing more general models
that would predict shifts in business over time. At the moment,
however, Hutchins feels that thescorecard is still early in its dev
elopment and current efforts are focused on identifying leading
indicators.
Hospital-Specific Analytical Activities—
Brigham and Women’s Hospital
26. Like MGH, the Brigham’s analytical activities in the past have
been largely focused on clinical research. Today it is also addre
ssing much ofthe same business, operational, and meaningful us
e issues that MGH is. Many of the analytical activities at the Br
igham are pursued by theCenter for Clinical Excellence (CCE),
which was founded by Dr. Michael Gustafson in 2001. The cent
er has five functionally interrelatedsections, including
• Quality programs
• Patient safety
• Performance improvement
• Decision support systems (including all internal and external d
ata management and reporting activities)
• Analysis and planning (which oversees business plan develop
ment, ROI assessments for major investments, cost benchmarkin
g,asset utilization reporting, and support for strategic planning)
The CCE has close working relationships with the Brigham’s C
FO and finance organizations, the Brigham’s information syste
msorganization, the Partners Business Development and Plannin
g function, and other centers and medical departments at the Bri
gham.
One major difference between the Brigham and MGH (and most
other hospitals, for that matter) is that the Brigham established
a balancedscorecard beginning in 2000. It was based on a well-
established cultural orientation to operational and quality metric
s throughout thehospital. Richard Nesson, the Brigham CEO wh
o had partnered with CIO John Glaser to introduce the LMR and
CPOE systems, was also astrong advocate of information-
driven decision making on both the clinical and business sides o
f the hospital. The original systems thatNesson and Glaser had e
stablished also incorporated a reporting tool called EX, and a da
ta warehouse called CHASE (ComputerizedHospital Analysis Sy
stem for Efficiency). The analyses and data from these systems
formed the core of the Brigham’s balanced scorecard.
Before an effective scorecard could be developed, the Brigham
had to undertake considerable work on data definitions and man
agement.One analysis discovered, for example, that there were f
27. ive different definitions of the length of a patient stay circulatin
g in 11 differentreports. The chief medical officer at the time, D
r. Andy Whittemore, and the CCE’s Dr. Gustafson, a surgeon w
ho had just taken on qualitymeasurement issues at the Brigham,
addressed these data issues with a senior executive steering com
mittee and decided to present thedata in an easy-to-
digest scorecard.
Under the ongoing management of the CCE, the scorecard conta
ins a variety of financial, operational, and clinical metrics from
across thehospital. The choice of metrics is driven by a “strateg
y map”7 specifying the relationships among key variables that d
rive the performance ofthe hospital (see Figure 18.1). Unlike m
ost corporate strategy maps, financial performance variables are
at the bottom of the map ratherthan the top. In the scorecard its
elf, there are more than 50 specific measures in the hospital-
wide scorecard, and more detailed scorecardsfor particular depa
rtments, such as Nursing and Surgery. The scorecard has also be
en extended to Faulkner Hospital, a Partners institutionthat is m
anaged jointly with the Brigham.
Figure 18.1 Strategy map for Brigham & Women’s balanced sco
recard
Dr. Gary Gottlieb, the Brigham president from 1992 to 2009, wa
s the most aggressive user of the scorecard. He noted:
I review the balanced scorecard on a regular basis, because ther
e is specific data that is of interest to me. There are key metrics
Iexamine for trends and if they develop, then I analyze the data
to better understand what is going right or wrong. It is one view
,but an important one of our hospital. I can look at the balanced
scorecard and get information in another way, from a differentp
erspective than I can when I’m making rounds on a hospital unit
, or sitting in the meeting with chiefs.8
Gottlieb left the Brigham CEO role to become the CEO of Partn
ers overall in 2010. One of the primary initiatives in his new Pa
rtners role isto expand the degree of common systems throughou
t Partners, so that there can be common data and analytics throu
28. ghout theorganization. Perhaps one day all of Partners HealthCa
re System will be managed through one scorecard.
Notes
1. This and other details of the Partners LMR/CPOE systems are
derived from Richard Kesner, “Partners Healthcare System:Tra
nsforming Healthcare Services Delivery Through Information M
anagement,” Ivey School of Business Case Study (2009).
2. “CIRD, Clinical Informatics Research & Development,” http:
//www.partners.org/cird/.
3. PricewaterhouseCoopers, “Partners HealthCare: Using EHR
Data for Post-
market Surveillance of Drugs” (2009). http://pwchealth.com/cgi
-local/hregister.cgi/reg/partners_healthcare_case_study.pdf.
4. Healthcare Financial Management Association, “Developing
a Meaningful EHR,” http://www.hfma.org/Publications/Leaders
hip-Publication/Archives/Special-Reports/Spring-
2010/Developing-a-Meaningful-
EHR/, Part 3 of “Leadership Spring-
Summer 2010Report: Collaborating for Results.”
5. The 25 meaningful use criteria are described in “Eligible Pro
vider: ‘Meaningful Use’ Criteria,” by Jack Beaudoin, Healthcar
e IT News,December 30, 2009, http://www.healthcareitnews.co
m/news/eligible-provider-meaningful-use-criteria.
6. Robert S. Kaplan and David P. Norton, “The Balanced Scorec
ard: Measures that Drive Performance,” Harvard Business Revie
w (January– February 1992).
7. Robert S. Kaplan and David P. Norton, “Having Trouble With
Your Strategy? Then Map It,” Harvard Business Review (Septe
mber –October, 2000).
8. Ibid.
· Notebook
Davenport, T., & McNeill, D. (2014). Analytics in healthcare
and the life sciences: Strategies,implementation, methods, and
best practices. Retrieved from https://content.ashford.edu
29. LSE - FM474
Questions:
Below you will find a number of questions that I want you to
address in your analysis
(approximate % weighting of each question is provided in
parentheses).
1. Evaluate Chrysler’s past performance. Is there evidence of
mismanagement? (25%)
a. Evaluate Chrysler’s financial and operating performance
between 1980-1992.
What financial and investment policies did they pursue and
why? How
successful were they?
b. What should Chrysler’s capital structure look like? What
payout policies
should they pursue? How does that compare with the policies
pursued by
current management?
2. What is the intrinsic value of a share of Chrysler stock? How
does that value compare to
the market’s valuation? (45%)
• When it comes to the capital structure assumptions, one can
imagine a number of
different alternatives, for example
30. 1. Assume that the firms debt will be kept at some constant
amount D.
2. Assume that Chrysler will follow some specific borrowing
and repayment
schedule for a number of years, after which the leverage policy
will be kept
constant.
3. Evaluate the structure of Kerkorian’s proposed deal in detail.
Does it make sense? What
risks are involved? Use the downturn of 1988-1991 to model
another downturn scenario.
(30%)
Assumptions:
• Market risk premium: 6%
• Tax rate: 39%
• Deferred taxes should be added back, since it is a non-cash
expense. (This is tax that
we owe, but do not presently have to pay to the IRS)
• Equity in unconsolidated subsidiaries is strictly speaking not a
cash income, which
implies that it is not part of the free cash flow. The equity stake
is valuable, however,
and should therefore be added to the value of the firm somehow.
32. closing on the 12th, Chrysler shares had risen to $48.75.
Kerkorian was Chrysler’s largest shareholder,
owning 10%. Lee Iacocca, Chrysler’s former CEO who was
forced into retirement in 1992 by the board,
was backing the Kerkorian bid. The proposed $19.5 billion deal
was sketched out to include $2 billion in
Chrysler equity already held by Kerkorian and Iacocca, $3.5
billion from outside equity investors, $8.8
billion in bank debt, and $5.2 billion from Chrysler's own $7.6
billion in cash. The group planned to
suspend annual dividends, totaling $650 million a year, to help
finance the deal.
Chrysler had built up its cash balance from $3 billion to $7.6
billion from 1992 to 1994 with solid
performances in a number of divisions. CEO Robert Eaton
argued that a cash reserve of at least $7.5
billion, or $21.13 per share, should be kept as a cushion for the
next downturn in the industry. But
Kerkorian and Iacocca thought otherwise. In a news conference
shortly after the announcement, Iacocca
stated:
You just watch, it [the cash] will self-fulfill the prophecy. If
you keep saying, we
need $7.5 billion and it's just a cushion, then the union -- and I
know them like I know
my kids -- will say, 'We have a place to put that money.' They
will want part of [it]
baked into the UAW contract for three years.1
Kerkorian and Iacocca argued that Chrysler needed $2.5 billion
in cash and $2.5 billion in bank
lines of credit to survive the next recession. Alex Yemenidjian,
an executive at the Tracinda Corporation,
which was Kerkorian’s wholly owned investment vehicle,
33. summed up the position succinctly: "We
understand they want a cushion, we just believe the cushion is
too large."2
After an emergency board meeting, Chrysler issued an
announcement, saying it was "not for
sale." Eaton remarked, "We don't want to put Chrysler at risk.
We've worked hard to build this
company's financial strength, to increase shareholder value, and
to build the confidence of customers,
employees, dealers and suppliers. We have no desire to reverse
this process."3 Other observers were
less subtle about the proposal. "It's immoral," said a ranking
U.S. official with an Italian bank. "I believe
in enhancing shareholder value, but as a long-term concept
rather than a short-term grab for profits. This
could only happen in this country."4
1. As quoted in The Wall Street Journal, April 13, 1995.
2. Ibid.
3. Ibid.
4.
As quoted in The Detroit News, April 19, 1995.
This document is authorized for use only in Dr Angie
Andrikogiannopoulou's FM474M CEMS EXCHANGE at London
School of Economics and Political Science (LSE) from Dec
2019 to Jun
2020.
296-078 The Chrysler Takeover Attempt
34. 2
Company Background
Chrysler was incorporated in 1925 by Walter Percy Chrysler, a
former vice president of General
Motors (GM). Resigning from GM over policy differences,
Chrysler rescued the Maxwell Motor
Corporation from insolvency and designed its new Chrysler
automobile. First exhibited in 1924, the car
was an immediate success and before year's end, the company
had sold 32,000 cars and had earned more
than $4 million. By 1940, Chrysler had acquired Dodge and
Plymouth, controlled 25% of the domestic
market, and surpassed Ford to become the second largest
automaker in the industry behind GM.
Although it lost ground to Ford and GM in the ensuing decades,
Chrysler was still third among U.S. and
worldwide automakers by the end of the 1960s. But the 1970s
were not good to Chrysler, as the oil
shocks, inflation in the economy, and increased Japanese
competition all took their toll on the company.5
The Iacocca Years In 1974 losses totaled a massive $52 million,
and the next year's deficit was
five times that amount. After a brief respite in 1976 and 1977,
Chrysler incurred net losses of $205 million
in 1978 and $1.1 billion in 1979. In just one year, Chrysler’s
worldwide sales of motor vehicles fell by 1.6
million units.6 It took a complex set of negotiations with
creditors and unions as well as a $1.5 billion
government bailout to save Chrysler from bankruptcy in 1978.
Lee Iacocca, the charismatic CEO who
was hired shortly after being fired from the presidency of Ford,
presided over Chrysler's comeback with
35. a flair for communications and salesmanship. By 1981,
Chrysler was on its way back. Its fleet had
achieved the best corporate average fuel economy in the
industry at 25.5 miles per gallon, and its Aries
and Reliant models had both received the prestigious “Motor
Trend Car the Year” award. By 1983,
Chrysler had achieved the largest percentage increase in U.S.
retail sales of any major domestic car maker
(19% for cars and 11% for trucks). Earnings were positive
again in 1983 and the company repaid the
government loan seven years early.7
After its recovery in the early 1980's, Chrysler diversified. It
acquired Gulfstream Aerospace,
Finance America, and E.F. Hutton Credit Corporation, among
others. It also merged with American
Motors Corporation, acquired the Italian automaker
Lamborghini, and established several joint-ventures
with Mitsubishi and Samsung. But at the end of 1989, Chrysler
announced that it was scrapping its
holding-company structure (which was created just four years
earlier) to cut costs. Soon thereafter, it
announced it would try to sell Gulfstream and Electrospace
Systems, marking a humiliating end to the
company's diversification strategy.8
In 1991 Chrysler lost $759 million, its debt was junk rated, and
its pension plans were
underfunded by more than $4 billion. Domestically, Chrysler
was selling only one in twelve cars, as
opposed to one in every nine cars five years earlier. Critics
argued that Chrysler’s financial problems
were a direct result of failing to invest in new product
development in the mid 1980s.9 But by 1992, new
models were ready, and hopes were high for another recovery.
Fortunately, sales of the higher-margin
36. minivans (a product Chrysler virtually invented in 1984) were
strong, and its other new models were
earning good reviews. They were the low priced Dodge Shadow
and Plymouth Sundance; the high
performance Dodge Stealth; the Dodge Spirit and Plymouth
Acclaim sedans; and the Jeep Grand
Cherokee and Dodge Dakota V-8 trucks. Despite all this, the
board thought it was time for new
leadership. In 1992 they chose Robert Eaton, head of European
operations at GM, to replace Iacocca.
Eaton Takes Over Eaton's focus from the start was on
transforming Chrysler into a company
that could withstand downturns. Shortly after becoming
chairman, he told company managers, "My
5. International Directory of Company Histories, Volume 1.
6. Chrysler Annual Report, 1980.
7. For further information, see “Chrysler: Iacocca's Legacy,”
Harvard Business School Case No. 493-017.
8. Ingrassia, Paul, and White, Joseph B., Comeback, The Fall
and Rise of the American Automobile Industry. New York:
Simon & Schuster, 1994, p. 195.
9. Frank Washington, "LH, as in 'Last Hope'," Newsweek, June
29, 1992 as quoted in HBS case No. 493-017.
This document is authorized for use only in Dr Angie
Andrikogiannopoulou's FM474M CEMS EXCHANGE at London
School of Economics and Political Science (LSE) from Dec
2019 to Jun
2020.
37. The Chrysler Takeover Attempt 296-078
3
personal ambition is to be the first chairman to never lead a
Chrysler comeback."10 The early results were
good as the stock price soared in 1992 and 1993 on the heels of
the economic recovery. New product
development was accelerated even more, and good reviews came
out for the LH sedans, the Dodge
Neon, and the midsize Cirrus and Stratus models. Chrysler also
continued to dominate the minivan
segment. In one of Eaton’s first major product moves, the
company invested $2.6 billion on a complete
redesign of the minivan line -- more than any new-vehicle
development program in company history.
But as interest rates began to climb and the stock price
remained flat, Chrysler was forced to take
steps to mollify Kerkorian, who was the largest shareholder at
9%. Management boosted its dividend by
60%, announced a $1 billion share buyback, and diluted its
poison pill so that individual investors could
raise their stakes to 15%. Nevertheless, the share price
continued to fall. Between mid-December and the
April 12 Kerkorian bid, Chrysler’s stock price fell 16% -- a
drop of one-third from its peak of $53 in
January, 1994 (see Exhibit 2).11
The Tracinda Group
The 77-year-old Kerkorian was the son of poor Armenian
farmers from Fresno, California. He
made his first millions running commercial and military flights
during the 1950s and 1960s, many of
them between Los Angeles and Las Vegas. He bought and sold
38. properties in Las Vegas and eventually
pioneered the notion of building huge hotels and attracting
people who had never gambled before.
Enticing people to "play where they stay" was a new idea which
proved extremely successful.12 Another
large part of his estimated $2.5 billion net worth came from
timely acquisitions and disposals of
Hollywood studios, among them Columbia Pictures and
MGM/UA.
Kerkorian owned all of the Tracinda Corporation, which was
the holding company for his
Chrysler stock. He began purchasing Chrysler in 1990 in the
middle of the recession for $12.37 per share.
By 1995, he had spent about $676 million accumulating his
stake. At the closing market price of $48.75
the day of the announcement, Kerkorian’s 36 million shares
were worth nearly $1.8 billion.
Many analysts wondered whether Kerkorian was serious about
his intent to buy control of
Chrysler. Ownership of a heavy manufacturing entity was not
characteristic of his long investment
history.13 For his part, Iacocca, 70, stated that he would serve
only as an advisor to Chrysler if the deal
went through, saying, "after 47 years in Detroit, I don't want to
go back."14 But others were more
suspicious of his motives. One reporter commented: "It's
impossible to believe Mr. Iacocca's current
protestations that he doesn't want to run Chrysler again. He
never wanted to stop running it, and at the
very least a Kerkorian victory would leave him in charge of all
the major strategic decisions at the
company."15
The Auto Industry Cycle
39. Supply In the volatile auto industry, car companies can quickly
shift from making a lot of money
to posting big losses when sales drop. One reason for this is
that traditionally, auto companies built
enough production capacity to supply everyone who wanted a
car in a boom year. This maximized
profits in boom years but led to excess inventory problems in
bad years. Also, in good times they
received payments for cars as soon as they were assembled, and
did not have to pay parts suppliers for
10. As quoted in The Wall Street Journal, April 14, 1995.
11. The Economist Newspaper, April 15, 1995.
12. The Washington Post, April 14, 1995.
13. Los Angeles Times, April 14, 1995.
14. As quoted in The Wall Street Journal, April 13, 1995.
15. Paul Ingrassia, "What's Driving the Chrysler Deal," The
Wall Street Journal, April 19, 1995.
This document is authorized for use only in Dr Angie
Andrikogiannopoulou's FM474M CEMS EXCHANGE at London
School of Economics and Political Science (LSE) from Dec
2019 to Jun
2020.
296-078 The Chrysler Takeover Attempt
4
up to 45 days. When sales sagged, however, auto makers ended
up paying for parts before the cars were
sold, straining cash reserves.16
40. To cover their high fixed costs when sales were flat, auto
makers cut their prices to move existing
inventory. These cuts, typically in the form of rebates and
dealer incentives, often escalated into
industry "incentive wars." Thus earnings would be more
variable than actual vehicle sales. For example,
from 1989 to 1990, Chrysler’s vehicle sales fell 16.8% from
2.38 to 1.98 million units. In that same period,
pretax income fell 74%, from $565 million to $147 million.
Likewise, when vehicle sales increased 11.5%
from 1993 to 1994, pretax income rose 51.9% in the same
period.
Demand Interest rates had a large impact on demand. As with
most companies, higher rates
increased the cost of capital and squeezed margins. But with
auto manufacturers, rising rates also had a
dramatic impact on consumer demand because buyers who
financed their auto purchases would have
higher monthly payments. Federal Reserve interest rate policy
was thus a key variable affecting the auto
cycle. Other key demand indicators were employment, real
income growth, the underlying age
composition of the motor vehicle fleet, and the strength of the
dollar relative to the currencies of Japan
and Europe.
The consensus among analysts in early 1995 was that new
vehicle sales would be sluggish
because of the recent Federal Reserve rate hikes and an overall
slowing of the economy. Some believed
that the auto cycle had already peaked, predicting that 1994
volumes would be very difficult to match. A
downturn was inevitable, they argued, and it was more likely to
come sooner rather than later. But
41. others believed that slower demand growth (rather than an
actual decline in demand) would lead to a
longer, flatter cycle for the auto companies. In this scenario,
Chrysler’s sales volumes would be
maintained by the pent-up demand still lingering from the last
recession.
Chrysler's Cash
When the 1989-1991 recession ended, management established
the goal of building up $5 billion
in cash to weather the next downturn. But when revenues
increased, Chrysler raised the target to $7.5
billion. As one official put it, "$7.5 billion would be prudent.
If you run the company with less cash, you
run a greater risk of having to cut product spending and pension
funding in the next downturn."17 But
in 1995 Chrysler’s pension was fully funded for the first time in
almost 40 years, and its credit rating had
just been upgraded to single-A by the major credit agencies.
Company plans called for an aggressive capital expenditure
program, projected to cost $3.2
billion in 1995 and $3.1 billion annually thereafter. Other
projected cash outlays included the $1 billion
stock buyback in 1995 (subject to “market conditions”), and
increasing the dividend payment from $1.00
to $1.60 per common share, adding about $200 million to the
annual cash outlay for dividends. In
addition, Chrysler’s stated goal was to lower its debt-to-capital
ratio from 18% to 10%. This would cost
approximately $1 billion, although the timing of the debt pay-
down was unknown.
On the product side, Chrysler was aggressively rolling out its
new models and predicting that
42. profit margins would improve as the product mix changed. But
some external factors were creating
uncertainty. Inventories for the Neon and the LH full-size
sedans were running above normal in the first
quarter. For the minivans, Chrysler was projecting the loss of
approximately 65,000 units during the
model changeover. Also, Ford was building its inventories to
uncomfortable levels, and all
manufacturers were adding capacity to the sport utility line
which included Chrysler’s high-margin
Grand Cherokee. The concern was that this could lead to price
cutting, followed by reduced margins.
16. The Wall Street Journal, April 17, 1995.
17. As quoted in The Wall Street Journal, April 17, 1995.
This document is authorized for use only in Dr Angie
Andrikogiannopoulou's FM474M CEMS EXCHANGE at London
School of Economics and Political Science (LSE) from Dec
2019 to Jun
2020.
The Chrysler Takeover Attempt 296-078
5
Finally, the crisis in Mexico was depressing sales there and
creating some uncertainty about the market
for the T300 pickup and the Cirrus/Stratus lines which were
manufactured in Mexico.
Deal Structure and Financing
43. For Tracinda, the structure of the deal would have an impact on
two key issues related to
Chrysler's cash position. First, the amount of cash they were
going to use from the company's balance
sheet would directly affect its ability to weather a future
downturn. Second, the deal structure itself
could have cash flow implications depending on the amount and
type of leverage used for the buyout.
Using $5.2 billion of Chrysler cash to finance the deal would
leave approximately $2.4 billion on
the balance sheet. Depending on projections of additional cash
build-up in the short term, Chrysler
would have anywhere from $2.5 billion to $4 billion to weather
the next downturn. As for the cash flow
implications of adding $8.8 billion of leverage, it appeared that
the after-tax cost of the additional interest
would be almost offset by the elimination of dividends.
Chrysler's finance subsidiary might also be available to support
some of the leverage in the deal.
Chrysler Financial (CFC) was a well-managed company with
earning assets to equity of roughly 4.5
times. This was much lower than GMAC (GM's finance unit)
which was at 9.0 times, and Ford Financial
Services which was at 9.6 times. Increasing leverage at
Chrysler Financial might provide an additional $2
billion in capital for the deal.
At the time of the announcement, Kerkorian had not yet
obtained financing for the deal. A
Tracinda spokesperson cited the need for secrecy as the reason
no banks had been contacted. But there
was some uncertainty about whether it could be raised at all.
One reason was that more than 150 banks -
- ranging from small local lenders to some of the world's
44. biggest banks -- were already tied up in
Chrysler credit agreements.
Reactions
As both sides in the deal stepped up the rhetoric on the
proposed takeover, Chrysler's analysts
remained mixed in their opinions. Summarizing the pro-
management stance, one analyst observed: "It's
really uncertainty in the economy that drove the stock down and
put Chrysler in play. And that is
completely out of Chrysler's control."18 These analysts were
convinced Chrysler represented a great
buying opportunity, with an inherent value in the range of $70
to $90 per share. David Cole, Director of
the Office for the Study of Automotive Transportation, was
even more bullish: “Wall Street has
undervalued the [auto] industry,” he said, placing the value of
Chrysler at $100 per share.19 But others
suggested that the large cash hoard and weak stock price were
signs that Chrysler wasn't handling its
finances properly. "The market is the ultimate arbiter on how
Chrysler is being run, and the market is
saying it's sorely mismanaged."20
Public reaction to the Tracinda group was mostly negative, as
many were calling the deal a
flashback to the excesses of the 1980s. The Tracinda team was
unmoved. Yemenidjian summarized the
group’s attitude: "We are the owners of the company. We are
not some outside intruders who came in to
spoil the company. The lack of respect is abominable."21
18. John Casesa of Wertheim Schroder, as quoted in The Wall
45. Street Journal, April 14, 1995.
19. As quoted in William J. Cook and Linda Grant, U.S. News
& World Report, April 24, 1995.
20. Analyst Nicholas Lobacarro of S.G. Warburg & Co., as
quoted in The Wall Street Journal, April 17, 1995.
21. As quoted in USA Today, April 27, 1995.
This document is authorized for use only in Dr Angie
Andrikogiannopoulou's FM474M CEMS EXCHANGE at London
School of Economics and Political Science (LSE) from Dec
2019 to Jun
2020.
296-078 The Chrysler Takeover Attempt
6
Exhibit 1 Chryslerís Board of Directors
Name Age Occupation Director Since
Lilyan H. Affinitok 63 Former Vice Chairman, Maxxam Group
1982
Robert E. Allen 60 Chairman and CEO, AT&T 1994
Joseph E. Antoninik 53 Former President and CEO, Kmart Corp.
1989
Joseph A. Califano, JR. k 63 Secretary of Health, Education,
and Welfare (1977-79) 1981
Thomas G. Denomme 55 Chrysler Vice Chairman 1993
Robert J. Eaton 55 Chrysler Chairman and CEO 1992
Earl G. Graves 60 Chairman and CEO, Earl G. Graves Ltd. 1990
Kent Kresa 57 Chairman and CEO, Northrop Grumman 1989
Robert J. Lanigan* 66 Chairman Emeritus, Owens-Illinois 1984
Robert A. Lutz 63 Chrysler President and Chief Operating
Officer 1986
46. Peter A. Magowan* 52 Chairman, Safeway 1986
Malcolm T. Stamper 69 Former Vice Chairman, Boeing 1984
Lynton R. Wilson 54 President and CEO, BCE Inc. 1984
kAlso a director of Kmart Corp.
*Both Lanigan and Magowan headed companies that were
acquired in leveraged buyouts by KKR.
Source: annual report.
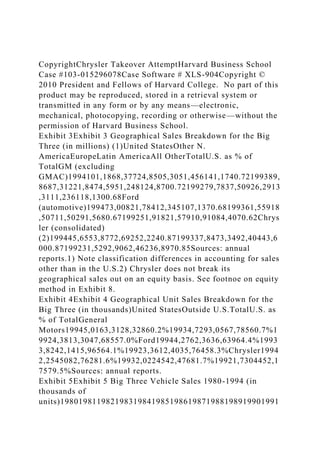
Exhibit 2 Big Three Closing Stock Prices and the S&P 500
Index, 1/3/95 to 4/12/95 (1/3/95 = 100)
77.00
79.00
81.00
83.00
85.00
87.00
89.00
91.00
93.00
95.00
97.00
99.00
101.00
103.00
105.00
107.00
109.00
111.00
1/
3/
51. The Chrysler Takeover Attempt 296-078
7
Exhibit 3 Geographical Sales Breakdown for the Big Three (in
millions) (1)
United Other Latin U.S. as %
States N. America Europe America All Other Total of Total
GM (excluding GMAC)
1994 101,186 8,377 24,850 5,305 1,456 141,174 0.72
1993 89,868 7,312 21,847 4,595 1,248 124,870 0.72
1992 79,783 7,509 26,291 3,311 1,236 118,130 0.68
Ford (automotive)
1994 73,008 21,784 12,345 107,137 0.68
1993 61,559 18,507 11,502 91,568 0.67
1992 51,918 21,579 10,910 84,407 0.62
Chrysler (consolidated) (2)
1994 45,655 3,877 2,692 52,224 0.87
1993 37,847 3,349 2,404 43,600 0.87
1992 31,529 2,906 2,462 36,897 0.85
Sources: annual reports.
1) Note classification differences in accounting for sales other
than in the U.S.
2) Chrysler does not break its geographical sales out on an
equity basis. See footnoe on equity method in Exhibit 8 .
52. Exhibit 4 Geographical Unit Sales Breakdown for the Big
Three (in thousands)
United Outside U.S. as %
States U.S. Total of Total
General Motors
1994 5,016 3,312 8,328 60.2%
1993 4,729 3,056 7,785 60.7%
1992 4,381 3,304 7,685 57.0%
Ford
1994 4,276 2,363 6,639 64.4%
1993 3,824 2,141 5,965 64.1%
1992 3,361 2,403 5,764 58.3%
Chrysler
1994 2,254 508 2,762 81.6%
1993 2,022 454 2,476 81.7%
1992 1,730 445 2,175 79.5%
Sources: annual reports.
This document is authorized for use only in Dr Angie
Andrikogiannopoulou's FM474M CEMS EXCHANGE at London
School of Economics and Political Science (LSE) from Dec
2019 to Jun
2020.
29
6-
07
8