Downloaded 15 times



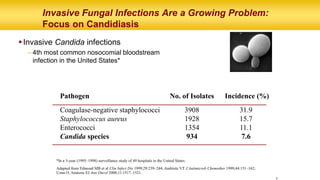
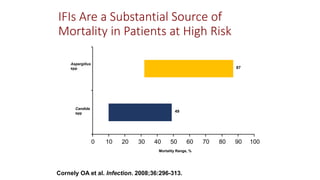
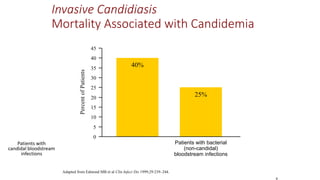







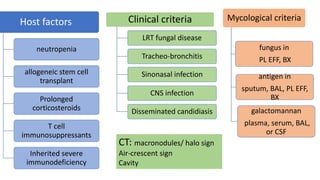
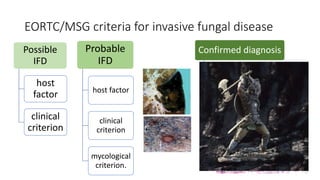
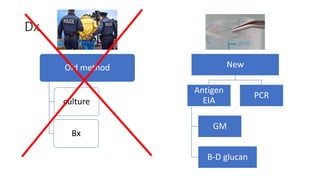
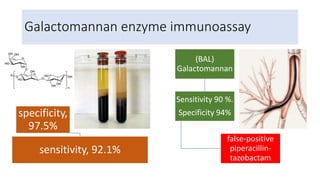
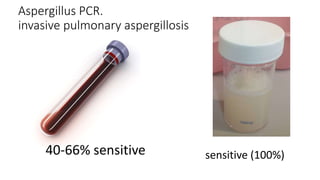
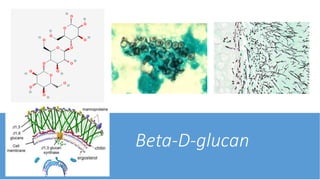




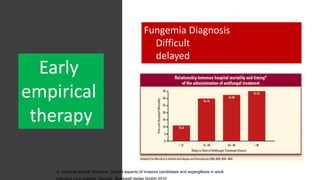




This document discusses fungal pulmonary infections. It begins by noting that fungi cause a small portion of community-acquired and hospital-acquired pneumonia cases. It then focuses on invasive fungal infections, noting that candidiasis is the fourth most common nosocomial bloodstream infection in the US. Mortality rates for invasive candidiasis and aspergillosis infections are also provided. The document provides information on diagnosing and treating various fungal infections like candidiasis, aspergillosis, and Pneumocystis jirovecii pneumonia. It discusses antifungal drug classes, specific drugs, and treatment guidelines.













































































